

Transcutaneous Electrical Acupoint Stimulation Reduces Postoperative Analgesic Requirement in Patients Undergoing Inguinal Hernia Repair: A Randomized, Placebo-Controlled Study
- PMID: 33406735
- PMCID: PMC7794768
- DOI: 10.3390/jcm10010146
Transcutaneous Electrical Acupoint Stimulation Reduces Postoperative Analgesic Requirement in Patients Undergoing Inguinal Hernia Repair: A Randomized, Placebo-Controlled Study
Abstract
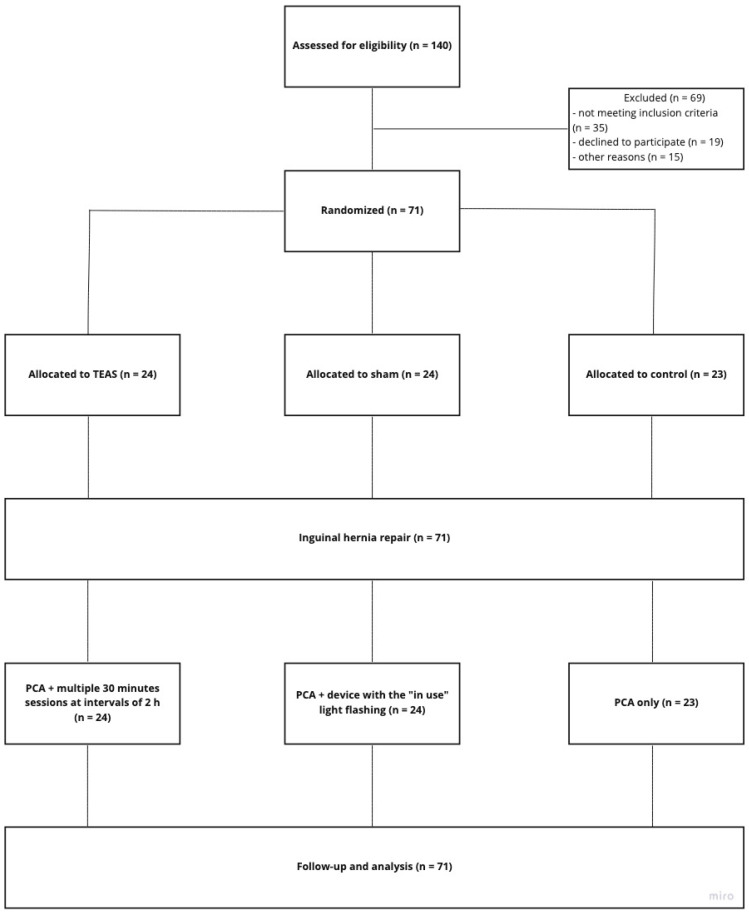
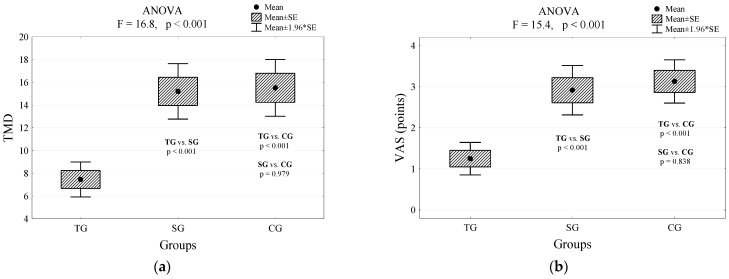
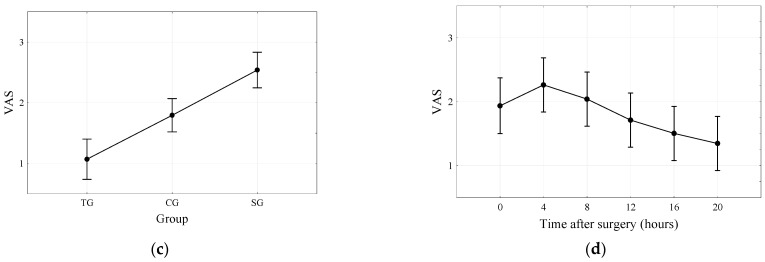
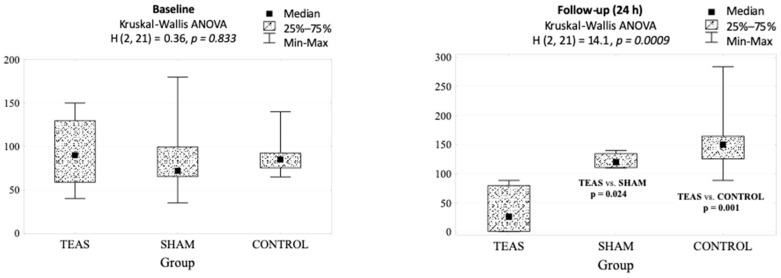
Given the rising rate of opioid-related adverse drug events during postsurgical pain management, a nonpharmacologic therapy that could decrease analgesic medication requirements would be of immense value. We designed a prospective, placebo-and-randomized controlled trial to assess the clinical effect of transcutaneous acupoint electrical stimulation (TEAS) on the postoperative patient-controlled analgesia (PCA) requirement for morphine, as well as side effects and recovery profile after inguinal hernia repair. Seventy-one subjects undergoing inguinal hernia repair with a standardized anesthetic technique were randomly assigned to one of three analgesic treatment regimens: PCA + TEAS (n = 24); PCA + sham-TEAS (no electrical stimulation) (n = 24), and PCA only (n = 23). The postoperative PCA requirement, pain scores, opioid-related side effects, and blood cortisol levels were recorded. TEAS treatment resulted in a twofold decrease in the analgesic requirement and decreased pain level reported by the patients. In addition, a significant reduction of cortisol level was reported in the TEAS group at 24 h postoperatively compared to the sham and control groups. We conclude that TEAS is a safe and effective option for reducing analgesic consumption and postoperative pain following inguinal hernia repair.
Keywords: TEAS; acupuncture; inguinal hernia; patient-controlled analgesia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Urman R.D., Seger D.L., Fiskio J.M., Neville B.A., Harry E.M., Weiner S.G., Lovelace B., Fain R., Cirillo J., Schnipper J.L. The Burden of Opioid-Related Adverse Drug Events on Hospitalized Previously Opioid-Free Surgical Patients. J. Patient Saf. 2019 doi: 10.1097/PTS.0000000000000566. - DOI - PubMed
-
- Shafi S., Collinsworth A.W., Copeland L.A., Ogola G.O., Qiu T., Kouznetsova M., Liao I.C., Mears N., Pham A.T., Wan G.J., et al. Association of opioid-related adverse drug events with clinical and cost outcomes among surgical patients in a large integrated health care delivery system. JAMA Surg. 2018;153:757–763. doi: 10.1001/jamasurg.2018.1039. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
