

Public health impact and cost effectiveness of routine and catch-up vaccination of girls and women with a nine-valent HPV vaccine in Japan: a model-based study
- PMID: 33407188
- PMCID: PMC7789539
- DOI: 10.1186/s12879-020-05632-0
Public health impact and cost effectiveness of routine and catch-up vaccination of girls and women with a nine-valent HPV vaccine in Japan: a model-based study
Abstract
Background: Combined with cancer screening programs, vaccination against human papillomavirus (HPV) can significantly reduce the high health and economic burden of HPV-related disease in Japan. The objective of this study was to assess the health impact and cost effectiveness of routine and catch-up vaccination of girls and women aged 11-26 years with a 4-valent (4vHPV) or 9-valent HPV (9vHPV) vaccine in Japan compared with no vaccination.
Methods: We used a mathematical model adapted to the population and healthcare settings in Japan. We compared no vaccination and routine vaccination of 12-16-year old girls with 1) 4vHPV vaccine, 2) 9vHPV vaccine, and 3) 9vHPV vaccine in addition to a temporary catch-up vaccination of 17-26 years old girls and women with 9vHPV. We estimated the expected number of disease cases and deaths, discounted (at 2% per year) future costs (in 2020 ¥) and discounted quality-adjusted life years (QALY), and incremental cost effectiveness ratios (ICER) of each strategy over a time horizon of 100 years. To test the robustness of the conclusions, we conducted scenario and sensitivity analyses.
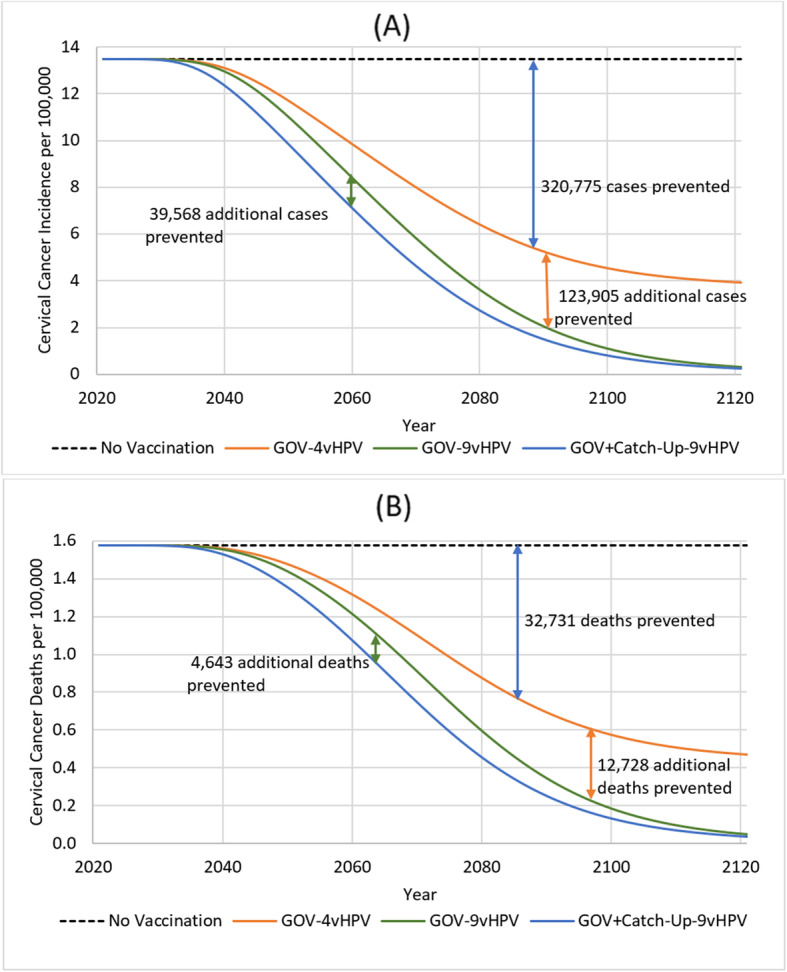
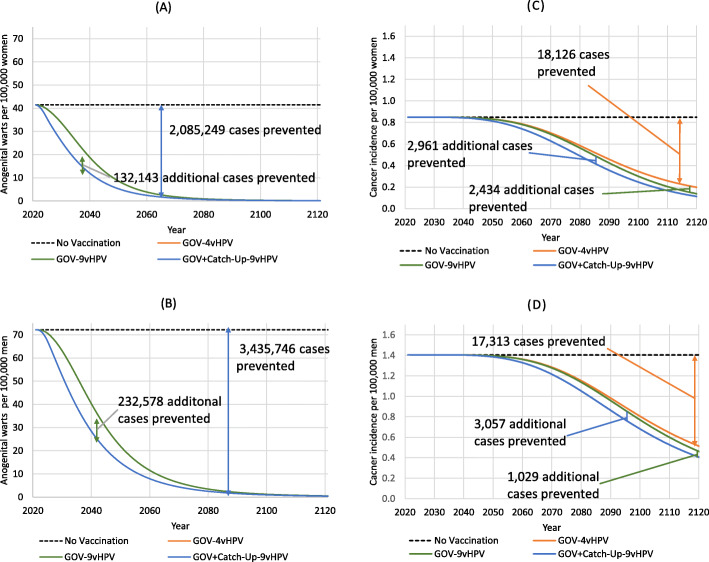
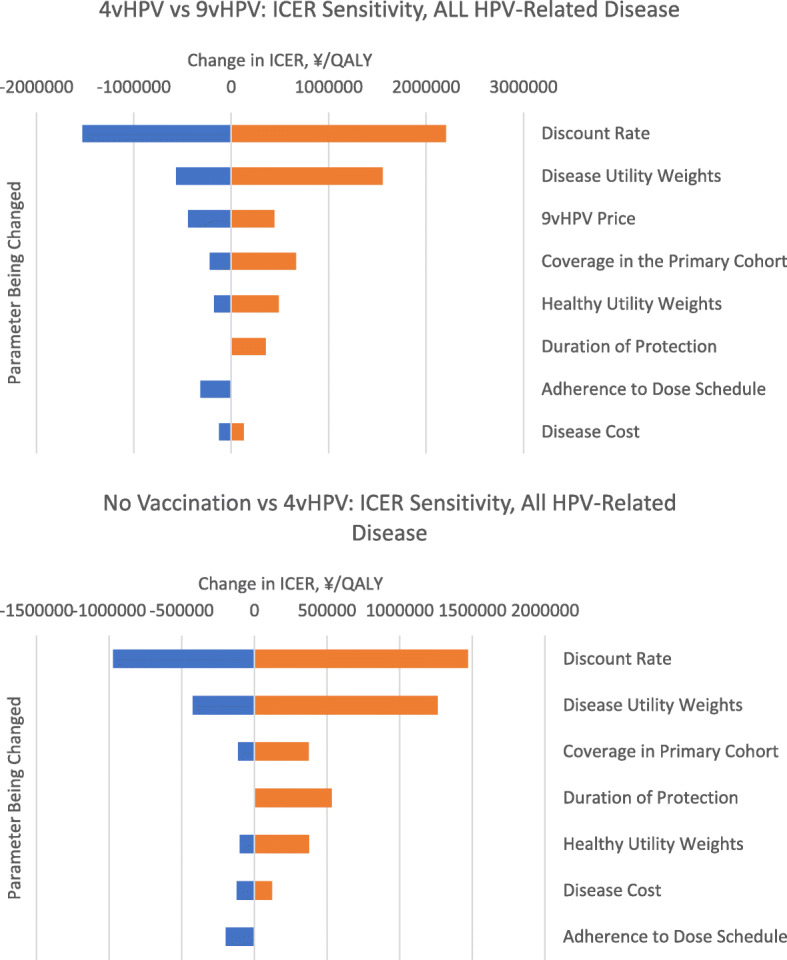
Results: Over 100 years, compared with no vaccination, 9vHPV vaccination was projected to reduce the incidence of 9vHPV-related cervical cancer by 86% (from 15.24 new cases per 100,000 women in 2021 to 2.02 in 2121). A greater number of cervical cancer cases (484,248) and cancer-related deaths (50,102) were avoided through the described catch-up vaccination program. Routine HPV vaccination with 4vHPV or 9vHPV vaccine prevented 5,521,000 cases of anogenital warts among women and men. Around 23,520 and 21,400 diagnosed non-cervical cancers are prevented by catch-up vaccination among women and men, respectively. Compared with no vaccination, the ICER of 4vHPV vaccination was ¥975,364/QALY. Compared to 4vHPV, 9vHPV + Catch-up had an ICER of ¥1,534,493/QALY.
Conclusions: A vaccination program with a 9-valent vaccine targeting 12 to 16 year-old girls together with a temporary catchup program will avert significant numbers of cases of HPV-related diseases among both men and women. Furthermore, such a program was the most cost effective among the vaccination strategies we considered, with an ICER well below a threshold of ¥5000,000/QALY.
Keywords: Anal; And oropharyngeal cancer; Cervical; Condylomata acuminate; Cost effectiveness analysis; Disease transmission models; Epidemiology; Genital warts; Herd protection/immunity; Human papillomavirus; Intraepithelial neoplasia; Japan; Oral cavity; Recurrent respiratory papillomatoses; Vaccines; Vaginal; Vulvar.
Conflict of interest statement
The 4-valent HPV vaccine, Gardasil® [Human Papillomavirus (Types 6, 11, 16,18) Recombinant Vaccine] and 9-valent HPV vaccine, Silgard9® [Human Papillomavirus (HPV 6, 11, 16, 18, 31, 33, 45, 52, and 58)] were developed and are currently marketed by Merck & Co., Inc., Kenilworth, NJ, USA. CP and EE are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. TK and AM are employees of MSD K.K., Tokyo, Japan.
Figures
Similar articles
-
The effects of human papillomavirus vaccination in Japan.Hum Vaccin Immunother. 2025 Dec;21(1):2489301. doi: 10.1080/21645515.2025.2489301. Epub 2025 Apr 11. Hum Vaccin Immunother. 2025. PMID: 40212002
-
Estimating the epidemiological impact and cost-effectiveness profile of a nonavalent HPV vaccine in Spain.Hum Vaccin Immunother. 2019;15(7-8):1949-1961. doi: 10.1080/21645515.2018.1560770. Epub 2019 Feb 20. Hum Vaccin Immunother. 2019. PMID: 30698488 Free PMC article.
-
The impact and cost-effectiveness of 9-valent human papillomavirus vaccine in adolescent females in Hong Kong.Cost Eff Resour Alloc. 2021 Nov 20;19(1):75. doi: 10.1186/s12962-021-00328-x. Cost Eff Resour Alloc. 2021. PMID: 34801050 Free PMC article.
-
Prophylaxis of cervical cancer and related cervical disease: a review of the cost-effectiveness of vaccination against oncogenic HPV types.J Manag Care Pharm. 2010 Apr;16(3):217-30. doi: 10.18553/jmcp.2010.16.3.217. J Manag Care Pharm. 2010. PMID: 20331326 Free PMC article. Review.
-
The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonavalent vaccine prevent?Euro Surveill. 2018 Oct;23(41):1700737. doi: 10.2807/1560-7917.ES.2018.23.41.1700737. Euro Surveill. 2018. PMID: 30326995 Free PMC article. Review.
Cited by
-
Vaccinating women previously treated for human papillomavirus-related cervical precancerous lesions is highly cost-effective in China.Front Immunol. 2023 Mar 27;14:1119566. doi: 10.3389/fimmu.2023.1119566. eCollection 2023. Front Immunol. 2023. PMID: 37051255 Free PMC article.
-
Screening for High-Risk Human Papillomavirus Reveals HPV52 and HPV58 among Pediatric and Adult Patient Saliva Samples.Dent J (Basel). 2024 Feb 29;12(3):56. doi: 10.3390/dj12030056. Dent J (Basel). 2024. PMID: 38534280 Free PMC article.
-
Cost-effectiveness analysis of single-dose or 2-dose of bivalent, quadrivalent, or nonavalent HPV vaccine in a low/middle-income country setting.J Gynecol Oncol. 2024 Nov;35(6):e85. doi: 10.3802/jgo.2024.35.e85. Epub 2024 Apr 18. J Gynecol Oncol. 2024. PMID: 38670561 Free PMC article.
-
Modelling epidemiological and economics processes - the case of cervical cancer.Health Econ Rev. 2025 Feb 22;15(1):13. doi: 10.1186/s13561-024-00589-1. Health Econ Rev. 2025. PMID: 39985694 Free PMC article. Review.
-
The impact of the COVID-19 pandemic on the national HPV immunization program in Malaysia.Front Public Health. 2022 Aug 1;10:907720. doi: 10.3389/fpubh.2022.907720. eCollection 2022. Front Public Health. 2022. PMID: 35979457 Free PMC article. Review.
References
-
- National Cancer Registry, Japan [https://ganjoho.jp/reg_stat/statistics/stat/summary.html ].
-
- Utada M, Chernyavskiy P, Lee WJ, Franceschi S, Sauvaget C, de Gonzalez AB, et al. Increasing risk of uterine cervical cancer among young Japanese women: comparison of incidence trends in Japan, South Korea and Japanese-Americans between 1985 and 2012. Int J Cancer. 2019;144(9):2144–2152. - PMC - PubMed
-
- Bruni L, Albero G, Serrano B, Mena M, Gómez D, Muñoz J, et al. Human papillomavirus and related diseases in United Kingdom. Summary report 17 June 2019. In., vol. 2020. United Kingdom: ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre); 2019.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
