

Clinical significance of D-dimer levels in refractory Mycoplasma pneumoniae pneumonia
- PMID: 33407216
- PMCID: PMC7787414
- DOI: 10.1186/s12879-020-05700-5
Clinical significance of D-dimer levels in refractory Mycoplasma pneumoniae pneumonia
Abstract
Background: The levels of serum D-dimer (D-D) in children with Mycoplasma pneumoniae pneumonia (MPP) were assessed to explore the clinical significance of D-D levels in refractory MPP (RMPP).
Method: A total of 430 patients with MPP were enrolled between January 2015 and December 2015 and divided into a general MPP (GMPP) group (n = 306) and a RMPP group (n = 124). Clinical data, D-D level, white blood cell (WBC) count, proportion of neutrophils (N%), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), alanine transaminase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) were compared between the two groups. Multivariate logistic regression was performed to identify independent predictors of RMPP.
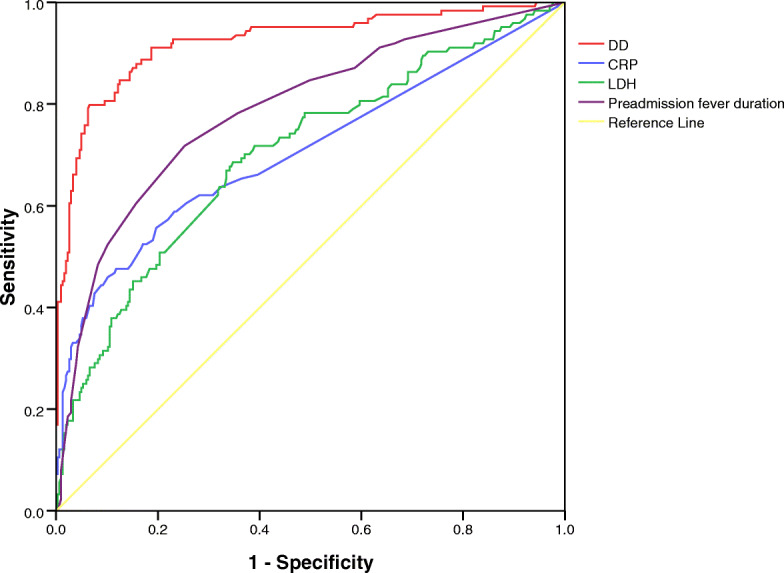
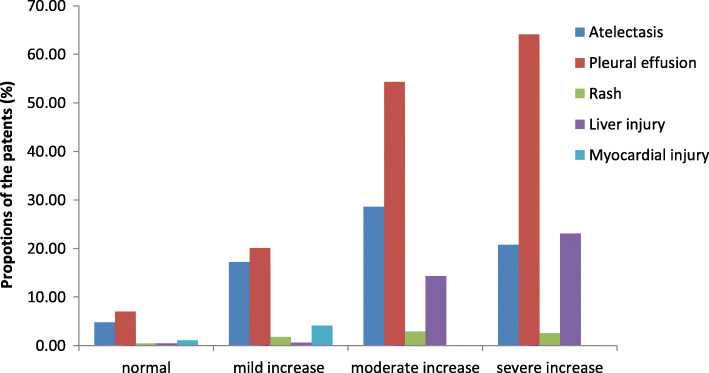
Results: (1) Hospitalization time, preadmission fever duration, total fever duration, WBC, N %, CRP, LDH, ESR, ALT, AST, and D-D were significantly higher in the RMPP group than those in the GMPP group (all P < 0.05). (2) Correlation analysis showed that D-D was positively correlated with WBC, CRP, ESR, and LDH, and could be used to jointly evaluate the severity of the disease. (3) Multivariate logistic regression analysis identified preadmission fever duration, CRP, LDH and DD as independent risk factors for RMPP (all P < 0. 05). D-D had the highest predictive power for RMPP (P < 0.01). The D-D level also had a good ability to predict pleural effusion and liver injury (all P < 0.01).
Conclusion: Serum D-D levels were significantly increased in patients with RMPP, indicating that excessive inflammatory response and vascular endothelial injury with prolonged duration existed in this patient population. Increased levels of serum D-D may be used as an early predictor of RMPP and the occurrence of complications. Our findings provide a theoretical basis for the early diagnosis of RMPP, early intervention and excessive inflammatory response in the pathogenesis of mycoplasma.
Keywords: Child; D-dimer; Mycoplasma pneumoniae; Refractory Mycoplasma pneumoniae pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ravelomanana L, Bouazza N, Rakotomahefa M, et al. Prevalence of mycoplasma pneumoniae infection in Malagasy children. Pediatr Infect Dis J. 2017;36(5):467–471. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
