

Myeloma cast nephropathy with diffuse amyloid casts without systemic amyloidosis: two cases report
- PMID: 33407225
- PMCID: PMC7789149
- DOI: 10.1186/s12882-020-02204-x
Myeloma cast nephropathy with diffuse amyloid casts without systemic amyloidosis: two cases report
Abstract
Background: Multiple myeloma (MM) is a plasma-cell derived hematologic malignant disease. The malignant proliferating plasma cells secrete massive monoclonal immunoglobulins which lead to various pathologic types of renal injury. Myeloma cast nephropathy (MCN) is the most common histopathologic lesion with the worst renal prognosis. Rarely, the free light chains in the protein casts can form amyloid fibrils. Here, we reported two rare cases of MCN with diffuse amyloid casts.
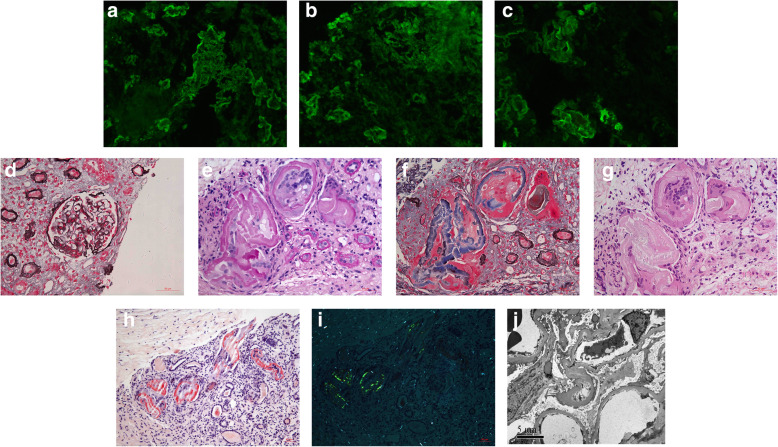
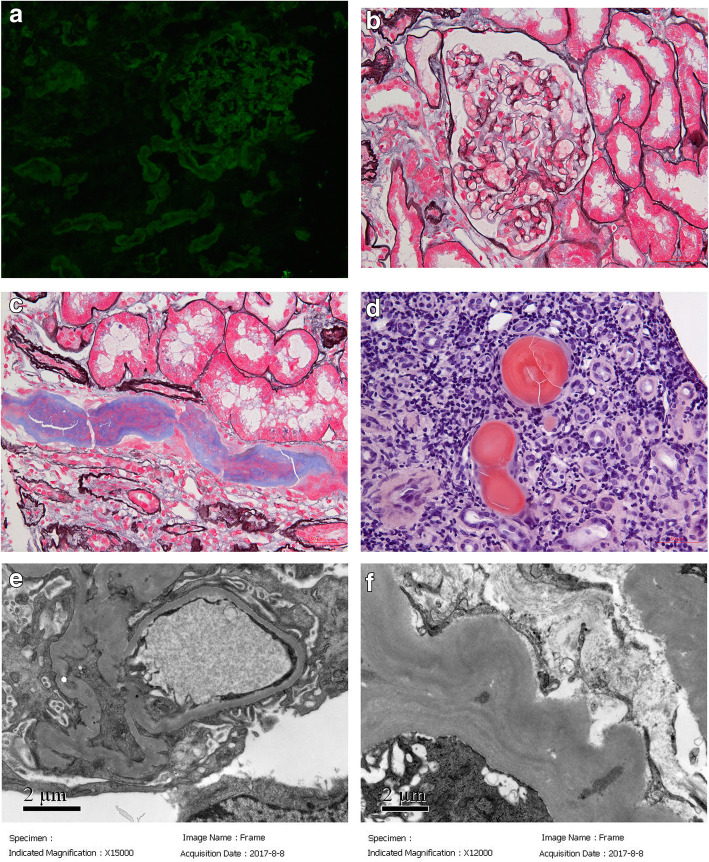
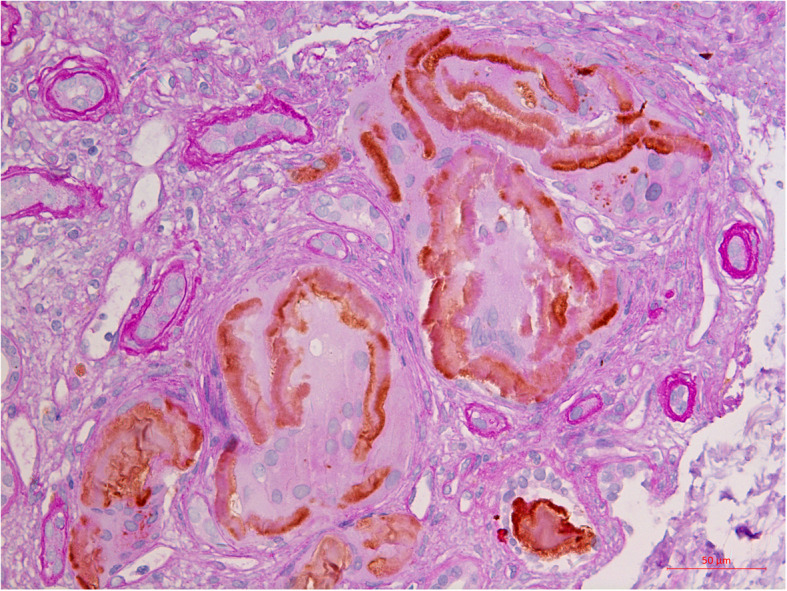
Case presentation: Case 1: A 54-year-old Chinese man presented with a 4-year history of multiple myeloma, proteinuria and hematuria. He had monoclonal IgAλ plus free λ spike in both serum and urine. He had been on chemotherapy for 4 years and maintained normal serum creatinine until 11 months ago. Then, his renal function deteriorated and he went on hemodialysis 4 months before admission. Renal biopsy showed diffuse amyloid casts in the tubular lumens, without any obvious amyloid deposits in other kidney compartments or signs of extra-renal amyloidosis. The amyloid fibrils formed around mononuclear cells which were CD68 negative. According to the morphology and location, these mononuclear cells were considered as tubular epithelial cells. The patient was maintained on chemotherapy and hemodialysis. He died 8 months after renal biopsy. Case 2: A 58-year-old Chinese man presented with a one-and-a-half-year history of proteinuria and slowly rising serum creatinine. He had monoclonal IgDλ spike in both serum and urine. Amyloid casts were observed in the tubular lumens and mononuclear cells could be identified in the center of some casts. There were no amyloid deposits in other kidney compartments and no sign of systemic amyloidosis. The patient also had fine granular deposits along the tubular basement membrane with λ linear staining along tubular basement membrane suggesting light chain deposition disease. He was treated with bortezomib-based chemotherapy followed by lenalidomide-based chemotherapy and achieved very good partial remission (VGPR). After 27 months of follow-up, the patient still showed no signs of systemic amyloidosis.
Conclusions: These 2 cases of MCN with diffuse amyloid casts have different histopathologic characteristics from the usual myeloma casts and tubular epithelial cells might play important roles in the pathogenesis.
Keywords: Amyloid; Multiple cast nephropathy; Multiple myeloma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clin Proc. 1975;50(1):29–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
