

Anti-synthetase syndrome: a rare and challenging diagnosis for bilateral ground-glass opacities-a case report with literature review
- PMID: 33407281
- PMCID: PMC7787399
- DOI: 10.1186/s12890-020-01388-0
Anti-synthetase syndrome: a rare and challenging diagnosis for bilateral ground-glass opacities-a case report with literature review
Abstract
Background: Anti-synthetase syndrome (ASS) is an uncommon immune-mediated entity characterized by myositis, interstitial lung disease (ILD), non-erosive arthritis, and less common features such as fever, Raynaud's phenomenon, and skin changes in association with anti-aminoacyl-transfer-RNA antibodies, most commonly anti-Jo-1 antibodies.
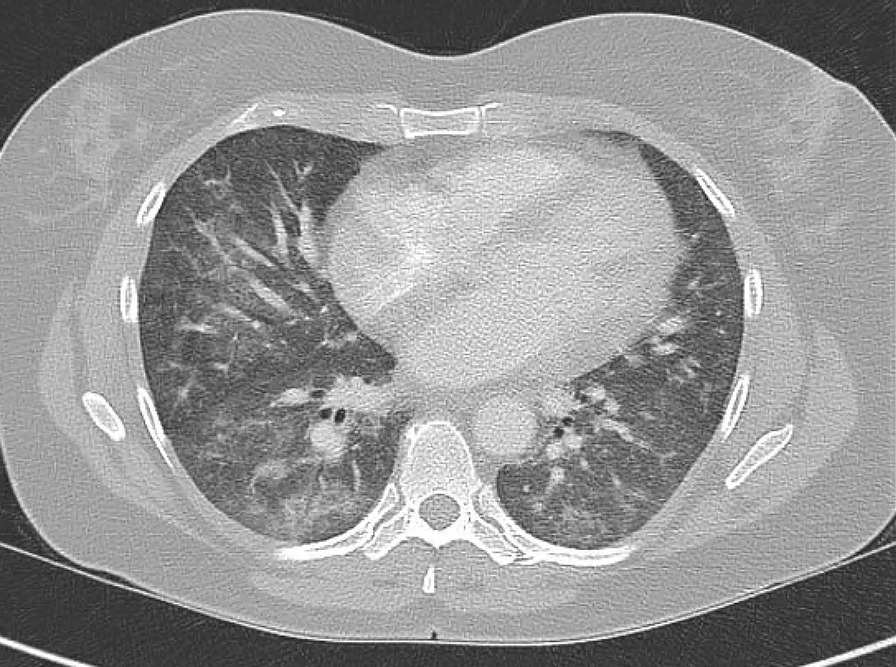
Case presentation: We present a challenging and rare case of ASS-associated ILD presenting with unexplained respiratory symptoms and bilateral infiltrates on chest imaging during the COVID-19 pandemic. High clinical suspicion for ASS with early appropriate therapy with corticosteroids and immunosuppressive agents led to marked clinical improvement.
Conclusion: High index of suspicion for ASS is mandated in patients with unexplained ILD. A comprehensive autoimmune work-up is important as an early treatment with corticosteroids with or without immunomodulators improves patient outcomes and survival in an otherwise poor prognostic disease.
Keywords: Anti-synthetase syndrome; Autoimmune disease; Corticosteroids; Interstitial lung disease.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- O'Hanlon TP, Carrick DM, Targoff IN, Arnett FC, Reveille JD, Carrington M, et al. Immunogenetic risk and protective factors for the idiopathic inflammatory myopathies: distinct HLA-A, -B, -Cw, -DRB1, and -DQA1 allelic profiles distinguish European American patients with different myositis autoantibodies. Medicine (Baltim) 2006;85(2):111–127. doi: 10.1097/01.md.0000217525.82287.eb. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
