

Imaging features of hemangioma in long tubular bones
- PMID: 33407312
- PMCID: PMC7786894
- DOI: 10.1186/s12891-020-03882-2
Imaging features of hemangioma in long tubular bones
Abstract
Background: To investigate the imaging features of hemangiomas in long tabular bones for better diagnosis.
Methods: Twenty-four patients with long bone hemangiomas confirmed by pathology were enrolled. Nineteen patients had plain radiography, fourteen patients had computed tomography (CT) and eleven had magnetic resonance imaging (MRI). The hemangioma was divided into medullary [13], periosteal [6] and intracortical type [5].
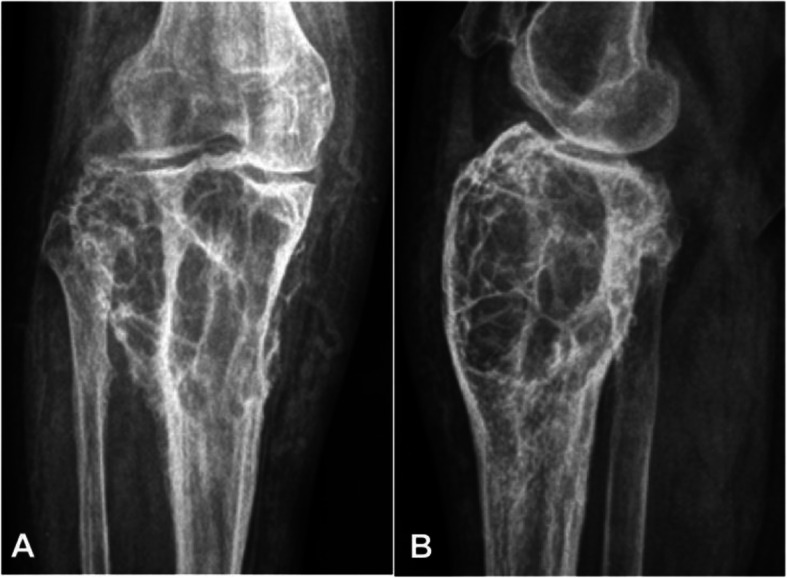
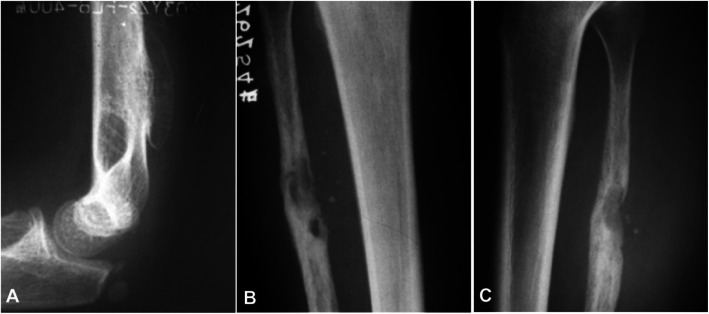
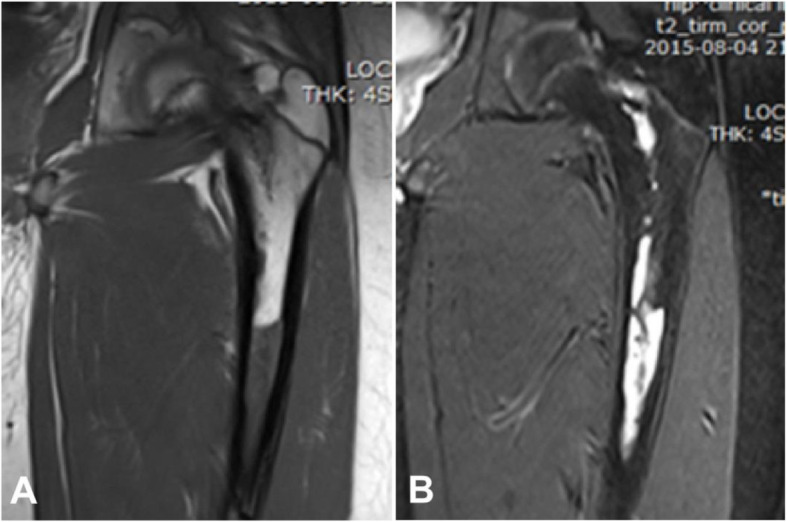
Results: Among 19 patients with plain radiography, eleven patients were medullary, three periosteal, and five intracortical. In the medullary type, the lesion was primarily osteolytic, including five cases with irregular and unclear rims and one lesion having osteosclerotic and unclear rims. In three patients with the periosteal type, the lesion had clear rims with involvement of the cortical bone in the form of bone defect, including two cases with local thickened bone periosteum and one case having expansile periosteum. Five intracortical hemangiomas had intracortical osteolytic lesions with clear margins. Among 14 patients with CT imaging, 8 cases were medullary, three periosteal, and three intracortical. Among 8 medullary hemangiomas, one had ground glass opacity, and seven had osteolytic, expansile lesions like soft tissue density with no calcification. In three periosteal cases, the lesion was osteolytic with thickened periosteum and narrowed medullary cavity. In three intracortical hemangiomas, the lesion was of even soft tissue density with no calcification. Among 11 patients with MRI imaging, seven were medullary, two periosteal, and two intracortical. Among 7 medullary lesions, six were of hypointense signal on T1WI and hyperintensesignal on T2 WI. In two periosteal cases, the periosteum was thickened, with one case being of equal signal, and the other having no signal. Two intracortical hemangiomas were both of slightly low signal on T1WI but hyperintense signal on T2WI.
Conclusions: The long bone hemangiomas had characteristic cystic honeycomb-like presentations in plain radiograph. CT and MRI imagings are helpful for diagnosis of hemangiomas in long bone.
Keywords: Computed tomography; Hamangioma; Long bone; Magnetic resonance imaging.; Plain radiography.
Conflict of interest statement
None
Figures


Similar articles
-
Clinical and Imaging Features of Desmoplastic Fibroma of Bone for Correct Diagnosis and Differentiation.Curr Med Imaging. 2022;18(10):1093-1098. doi: 10.2174/1573405618666220411125408. Curr Med Imaging. 2022. PMID: 35410618
-
Hemangiomas of the long tubular bone.Clin Orthop Relat Res. 1992 Jul;(280):256-60. Clin Orthop Relat Res. 1992. PMID: 1611755
-
Hemangioma of long tubular bone: imaging characteristics with emphasis on magnetic resonance imaging.Skeletal Radiol. 2020 Dec;49(12):2029-2038. doi: 10.1007/s00256-020-03527-4. Epub 2020 Jun 27. Skeletal Radiol. 2020. PMID: 32594199
-
Intraosseous hemangioma of the appendicular skeleton: imaging features of 15 cases, and a review of the literature.Skeletal Radiol. 2012 Dec;41(12):1525-36. doi: 10.1007/s00256-012-1444-z. Epub 2012 Jun 27. Skeletal Radiol. 2012. PMID: 22736082 Review.
-
Solitary skeletal hemangioma of the extremities.Skeletal Radiol. 2000 Sep;29(9):502-13. doi: 10.1007/s002560000251. Skeletal Radiol. 2000. PMID: 11000295 Review.
Cited by
-
Quantitative and Comparative Analysis of Effectivity and Robustness for Enhanced and Optimized Non-Local Mean Filter Combining Pixel and Patch Information on MR Images of Musculoskeletal System.Sensors (Basel). 2021 Jun 17;21(12):4161. doi: 10.3390/s21124161. Sensors (Basel). 2021. PMID: 34204477 Free PMC article.
-
Revisiting Fat Content in Bone Lesions: Paradigms in Bone Lesion Detection.Diseases. 2025 Jun 27;13(7):197. doi: 10.3390/diseases13070197. Diseases. 2025. PMID: 40709987 Free PMC article. Review.
-
Displaced humeral pathological fracture secondary to intraosseous hemangioma.Radiol Case Rep. 2022 Mar 18;17(5):1609-1613. doi: 10.1016/j.radcr.2022.02.020. eCollection 2022 May. Radiol Case Rep. 2022. PMID: 35313567 Free PMC article.
-
Bone lesions of the tibia: Multimodal iconographic review and diagnostic algorithms, Part 2: Metaphyseal and epiphyseal lesions.Eur J Radiol Open. 2025 May 1;14:100654. doi: 10.1016/j.ejro.2025.100654. eCollection 2025 Jun. Eur J Radiol Open. 2025. PMID: 40395360 Free PMC article. Review.
-
Management of a Rare Case of Cavernous Medullary Intraosseous Hemangioma in Proximal Tibia of a 38-year-old Female.J Orthop Case Rep. 2022;12(5):96-100. doi: 10.13107/jocr.2022.v12.i05.2834. J Orthop Case Rep. 2022. PMID: 36660152 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
