

Incidence and clinical impact of vertebral endplate changes after limited lumbar microdiscectomy and implantation of a bone-anchored annular closure device
- PMID: 33407349
- PMCID: PMC7788762
- DOI: 10.1186/s12893-020-01011-3
Incidence and clinical impact of vertebral endplate changes after limited lumbar microdiscectomy and implantation of a bone-anchored annular closure device
Abstract
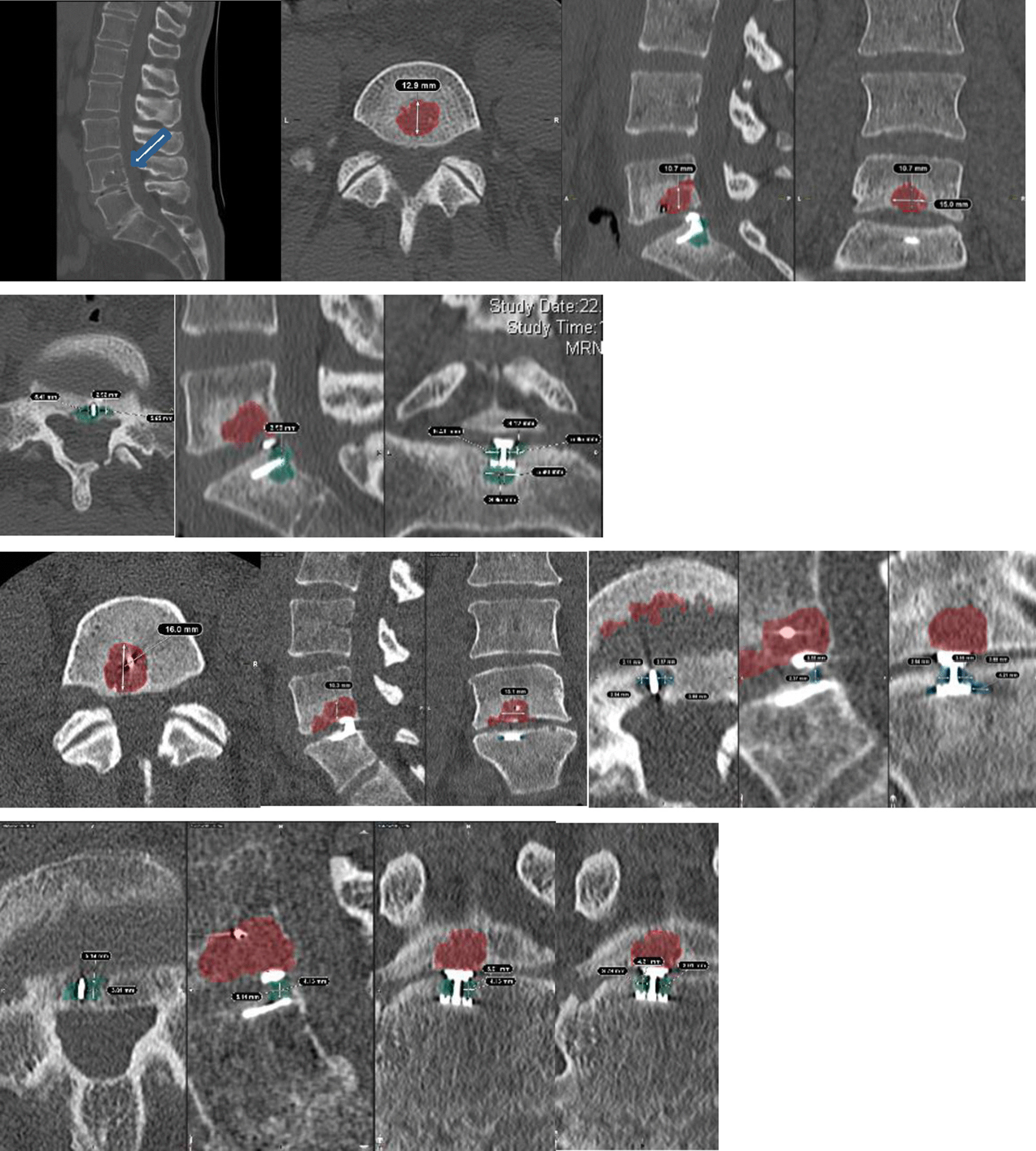
Background: An annular closure device (ACD) could potentially prevent recurrent herniation by blocking larger annular defects after limited microdiscectomy (LMD). The purpose of this study was to analyze the incidence of endplate changes (EPC) and outcome after LMD with additional implantation of an ACD to prevent reherniation.
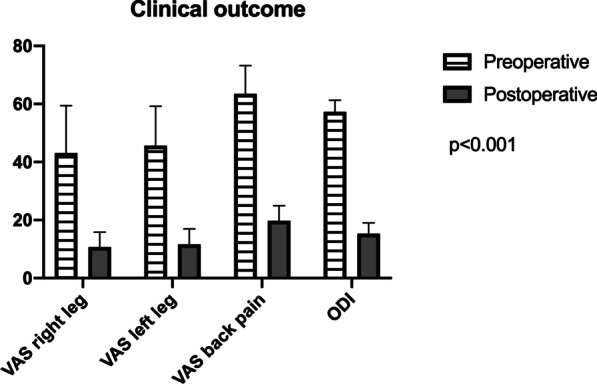
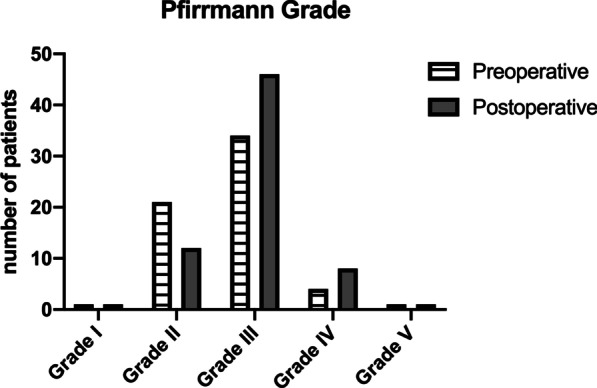
Methods: This analysis includes data from a) RCT study-arm of patients undergoing LMD with ACD implantation and b) additional patients undergoing ACD implantation at our institution. Clinical findings (VAS, ODI), radiological outcome (reherniation, implant integrity, volume of EPC) and risk factors for EPC were assessed.
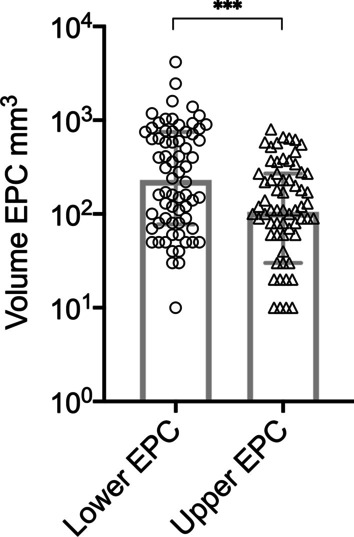
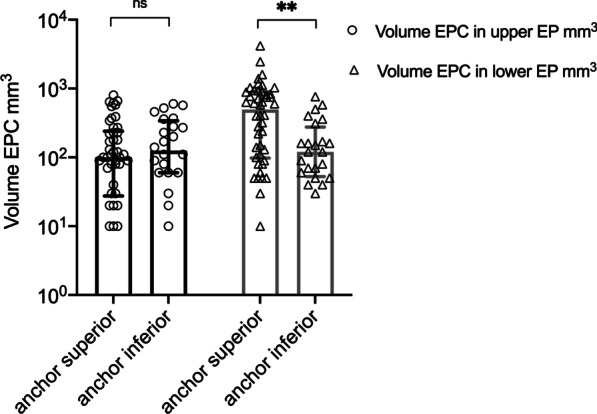
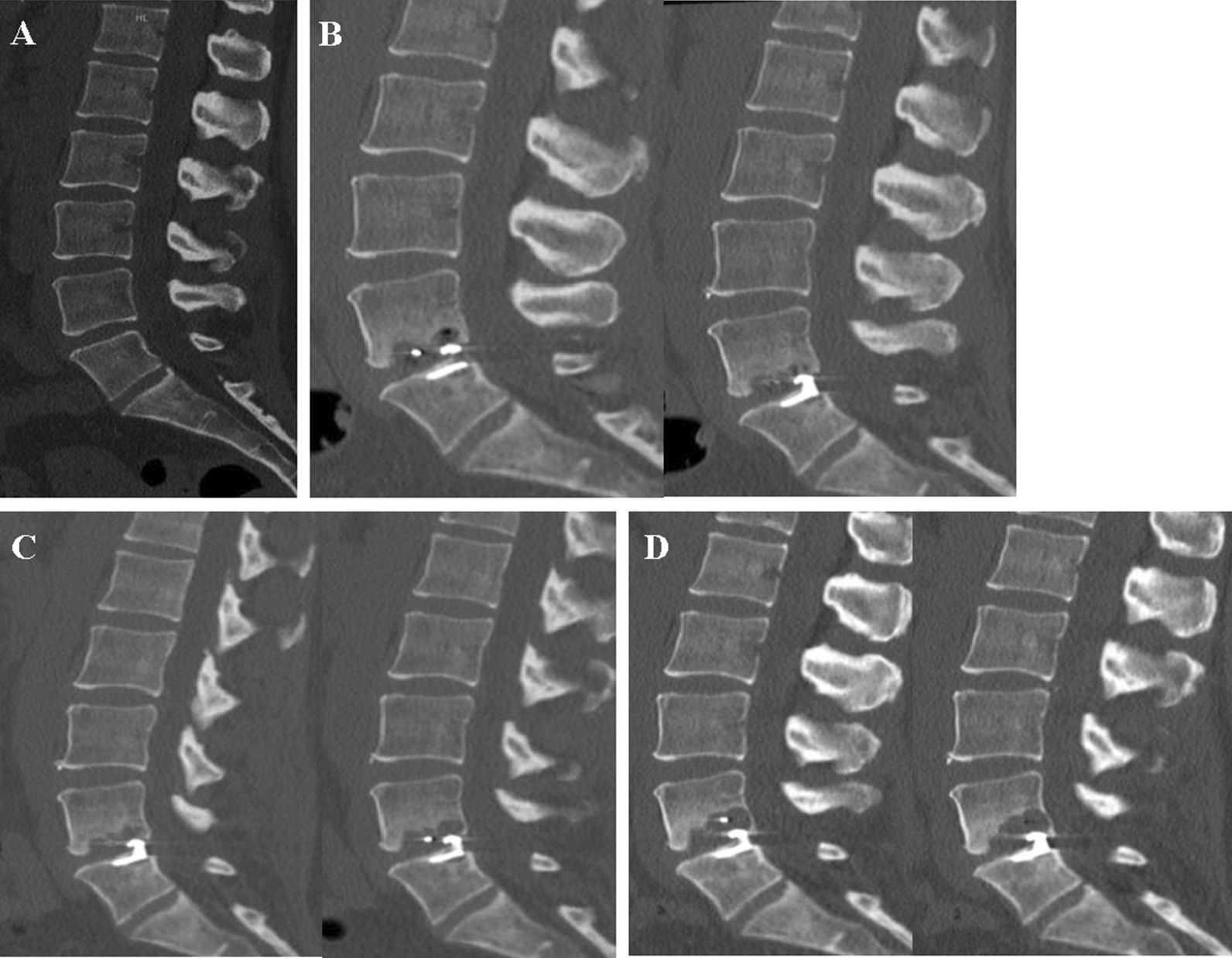
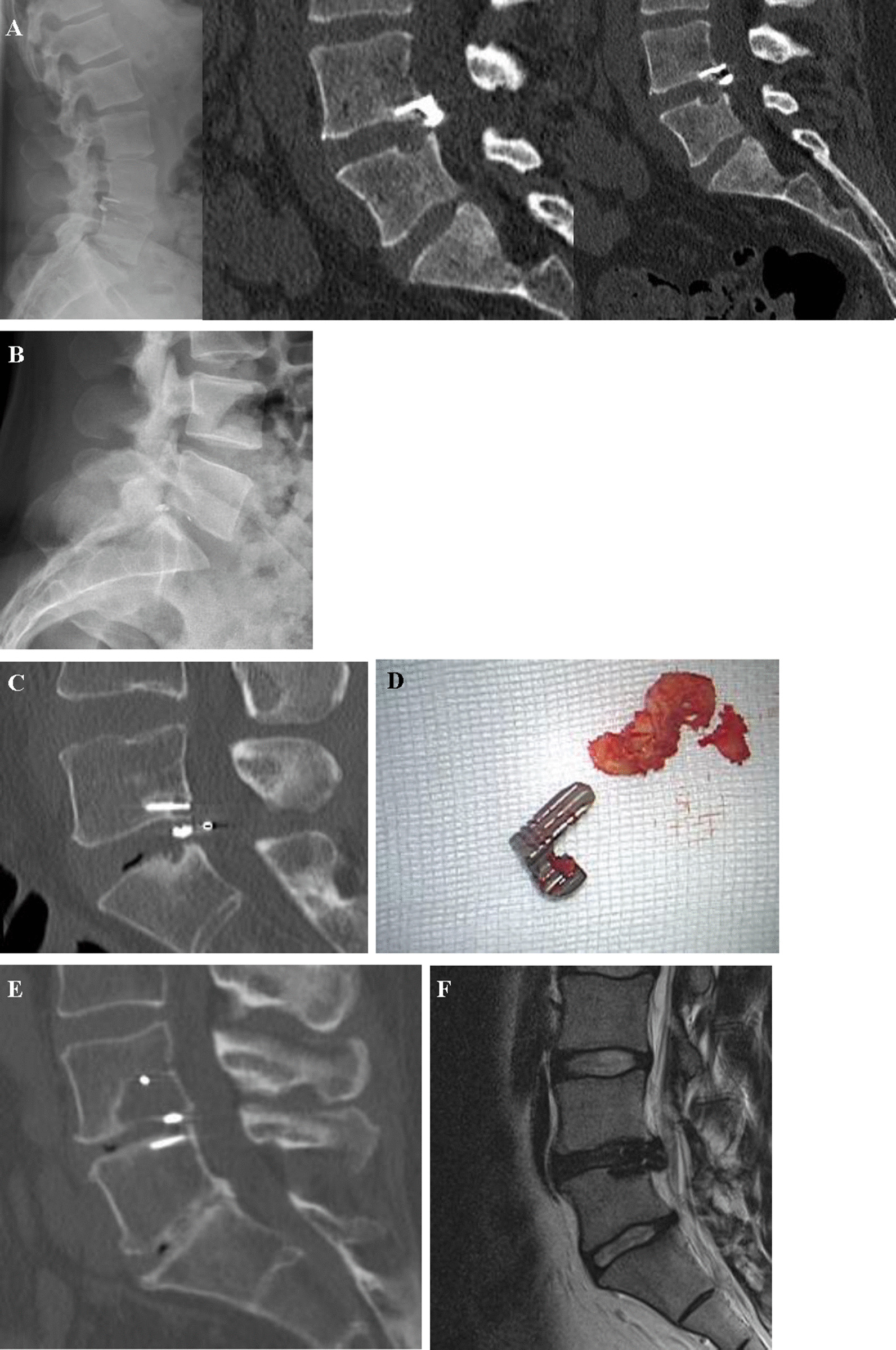
Results: Seventy-two patients (37 men, 47 ± 11.63yo) underwent LMD and ACD implantation between 2013-2016. A total of 71 (99%) patients presented with some degree of EPC during the follow-up period (14.67 ± 4.77 months). In the multivariate regression analysis, localization of the anchor was the only significant predictor of EPC (p = 0.038). The largest EPC measured 4.2 cm3. Reherniation was documented in 17 (24%) patients (symptomatic: n = 10; asymptomatic: n = 7). Six (8.3%) patients with symptomatic reherniation underwent rediscectomy. Implant failure was documented in 19 (26.4%) patients including anchor head breakage (n = 1, 1.3%), dislocation of the whole device (n = 5, 6.9%), and mesh dislocation into the spinal canal (n = 13, 18%). Mesh subsidence within the EPC was documented in 15 (20.8%) patients. Seven (9.7%) patients underwent explantation of the entire, or parts of the device.
Conclusion: Clinical improvement after LMD and ACD implantation was proven in our study. High incidence and volume of EPC did not correlate with clinical outcome. The ACD might prevent disc reherniation despite implant failure rates. Mechanical friction of the polymer mesh with the endplate is most likely the cause of EPC after ACD.
Keywords: Annular closure device; Barricaid®; Disc herniation; Endplate changes; Polymer mesh; Reherniation.
Conflict of interest statement
None of the authors had any conflicts of interest. No disclosures need to be made.
Figures


References
-
- Aizawa T, Ozawa H, Kusakabe T, Nakamura T, Sekiguchi A, Takahashi A, Sasaji T, Tokunaga S, Chiba T, Morozumi N, Koizumi Y, Itoi E. Reoperation for recurrent lumbar disc herniation: a study over a 20-year period in a Japanese population. J Orthop Sci. 2012;17:107–113. doi: 10.1007/s00776-011-0184-6. - DOI - PubMed
-
- Ambrossi GL, McGirt MJ, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL, Long DM (2009) Recurrent lumbar disc herniation after single-level lumbar discectomy: incidence and health care cost analysis. Neurosurgery 65:574–578 (discussion 578) doi: 10.1227/01.NEU.0000350224.36213.F9 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
