

Minimally disruptive medicine (MDM) in clinical practice: a qualitative case study of the human immunodeficiency virus (HIV) clinic care model
- PMID: 33407451
- PMCID: PMC7788961
- DOI: 10.1186/s12913-020-06010-x
Minimally disruptive medicine (MDM) in clinical practice: a qualitative case study of the human immunodeficiency virus (HIV) clinic care model
Abstract
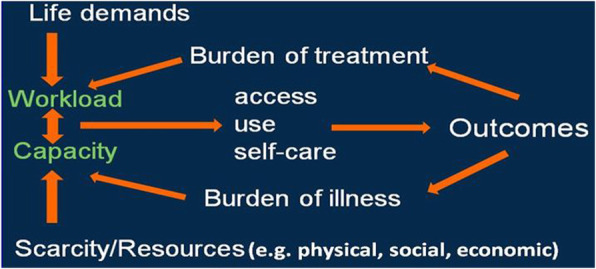
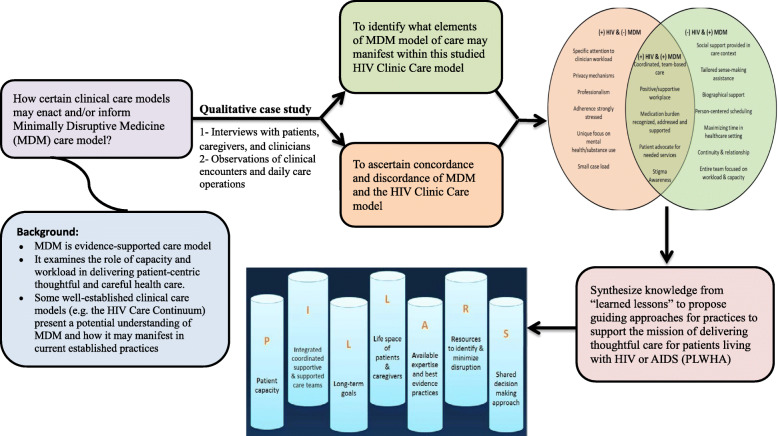
Background: Recent evidence suggests the need to reframe healthcare delivery for patients with chronic conditions, with emphasis on minimizing healthcare footprint/workload on patients, caregivers, clinicians and health systems through the proposed Minimally Disruptive Medicine (MDM) care model named. HIV care models have evolved to further focus on understanding barriers and facilitators to care delivery while improving patient-centered outcomes (e.g., disease progression, adherence, access, quality of life). It is hypothesized that these models may provide an example of MDM care model in clinic practice. Therefore, this study aimed to observe and ascertain MDM-concordant and discordant elements that may exist within a tertiary-setting HIV clinic care model for patients living with HIV or AIDS (PLWHA). We also aimed to identify lessons learned from this setting to inform improving the feasibility and usefulness of MDM care model.
Methods: This qualitative case study occurred in multidisciplinary HIV comprehensive-care clinic within an urban tertiary-medical center. Participants included Adult PLWHA and informal caregivers (e.g. family/friends) attending the clinic for regular appointments were recruited. All clinic staff were eligible for recruitment. Measurements included; semi-guided interviews with patients, caregivers, or both; semi-guided interviews with varied clinicians (individually); and direct observations of clinical encounters (patient-clinicians), as well as staff daily operations in 2015-2017. The qualitative-data synthesis used iterative, mainly inductive thematic coding.
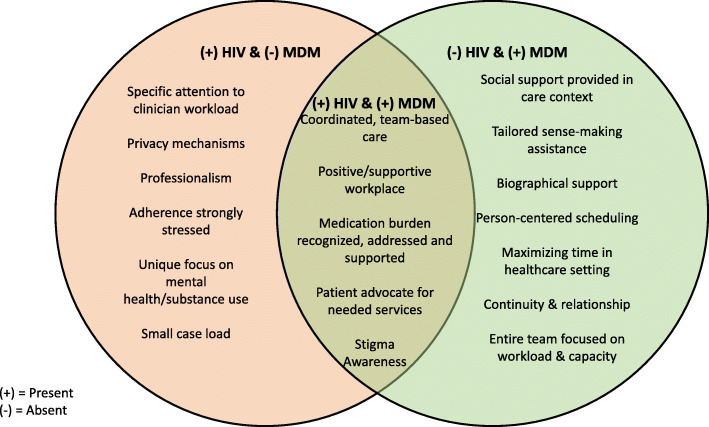
Results: Researcher interviews and observations data included 28 patients, 5 caregivers, and 14 care-team members. With few exceptions, the clinic care model elements aligned closely to the MDM model of care through supporting patient capacity/abilities (with some patients receiving minimal social support and limited assistance with reframing their biography) and minimizing workload/demands (with some patients challenged by the clinic hours of operation).
Conclusions: The studied HIV clinic incorporated many of the MDM tenants, contributing to its validation, and informing gaps in knowledge. While these findings may support the design and implementation of care that is both minimally disruptive and maximally supportive, the impact of MDM on patient-important outcomes and different care settings require further studying.
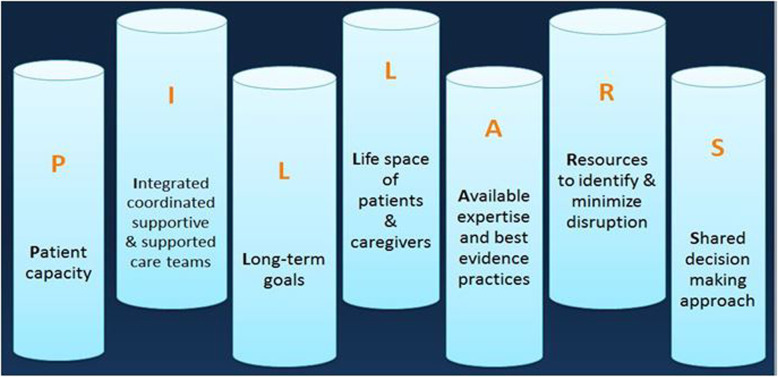
Keywords: Capacity; Cumulative complexity model; HIV care; Healthcare burden; MDM; Minimally disruptive medicine; Model of care; PILLARS; Treatment burden; Workload.
Conflict of interest statement
No conflict of or competing interests reported for all authors.
Figures
References
-
- May C, Montori VM, Mair FS. We need minimally disruptive medicine. BMJ. 2009;339:b2803. - PubMed
-
- Abu Dabrh AM, Gallacher K, Boehmer KR, Hargraves IG, Mair FS. Minimally disruptive medicine: the evidence and conceptual progress supporting a new era of healthcare. J R Coll Physicians Edinb. 2015;45(2):114–117. - PubMed
-
- Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012;65(10):1041–1051. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
