

Deep learning model for classifying endometrial lesions
- PMID: 33407588
- PMCID: PMC7788977
- DOI: 10.1186/s12967-020-02660-x
Deep learning model for classifying endometrial lesions
Abstract
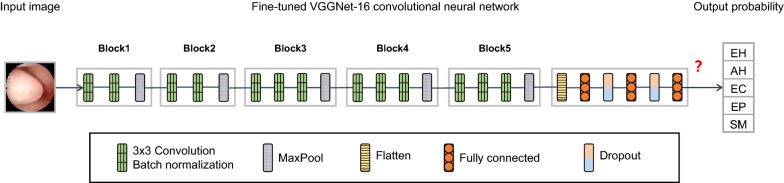
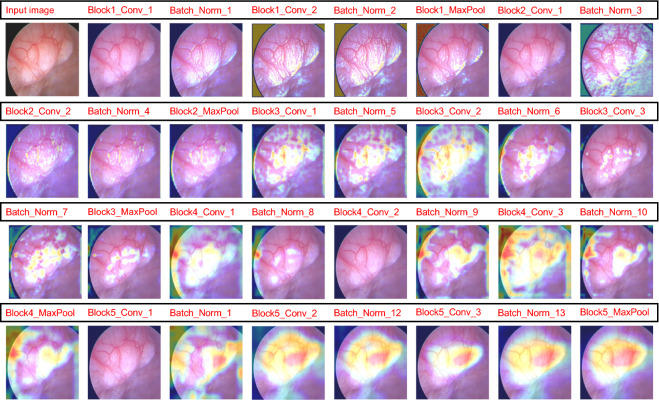
Background: Hysteroscopy is a commonly used technique for diagnosing endometrial lesions. It is essential to develop an objective model to aid clinicians in lesion diagnosis, as each type of lesion has a distinct treatment, and judgments of hysteroscopists are relatively subjective. This study constructs a convolutional neural network model that can automatically classify endometrial lesions using hysteroscopic images as input.
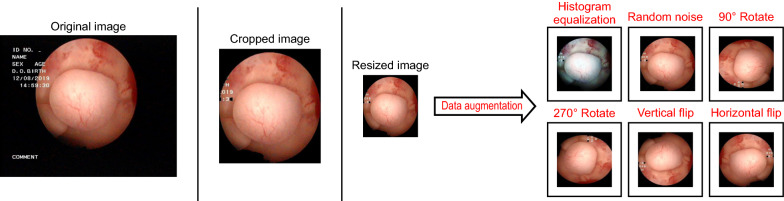
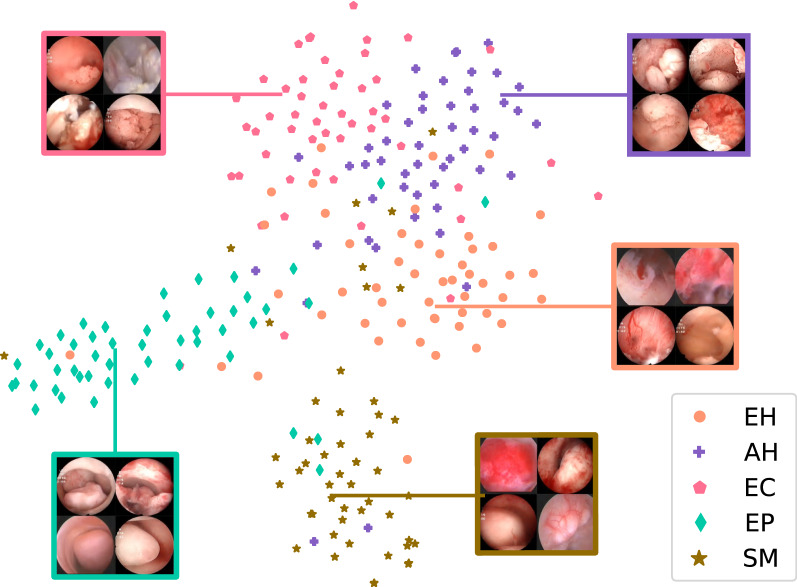
Methods: All histopathologically confirmed endometrial lesion images were obtained from the Shengjing Hospital of China Medical University, including endometrial hyperplasia without atypia, atypical hyperplasia, endometrial cancer, endometrial polyps, and submucous myomas. The study included 1851 images from 454 patients. After the images were preprocessed (histogram equalization, addition of noise, rotations, and flips), a training set of 6478 images was input into a tuned VGGNet-16 model; 250 images were used as the test set to evaluate the model's performance. Thereafter, we compared the model's results with the diagnosis of gynecologists.
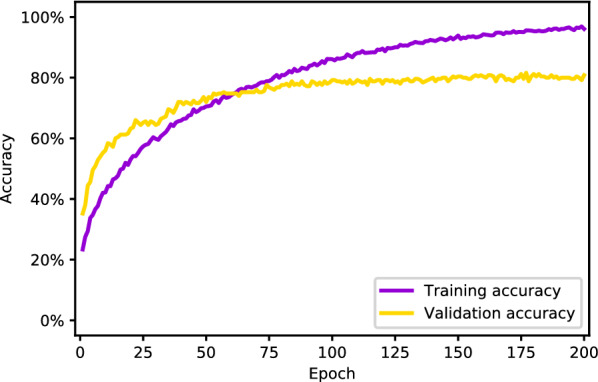
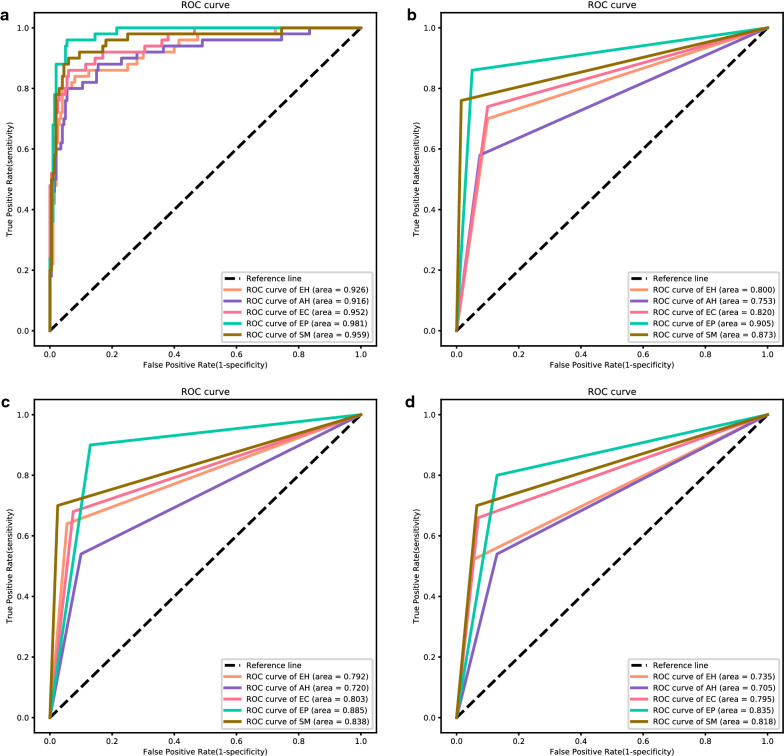
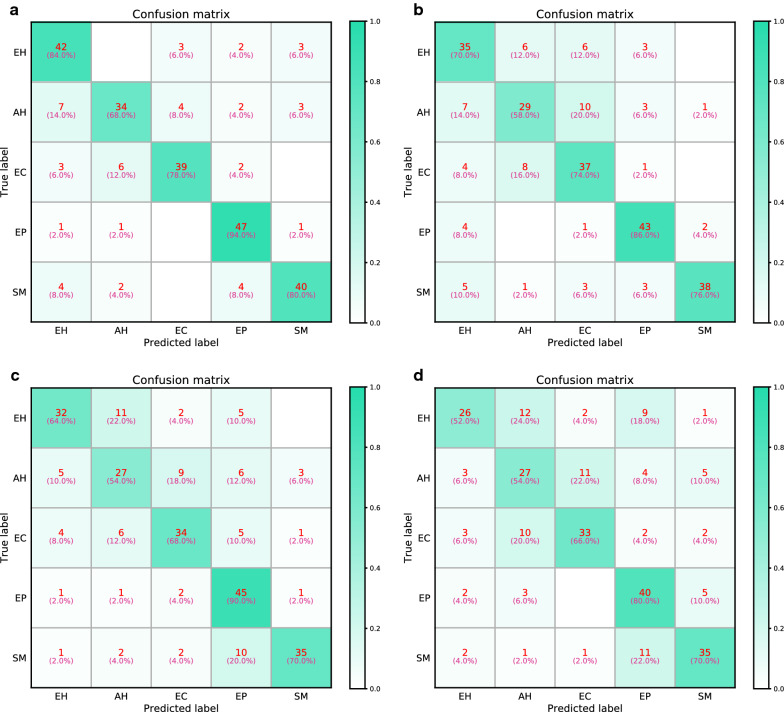
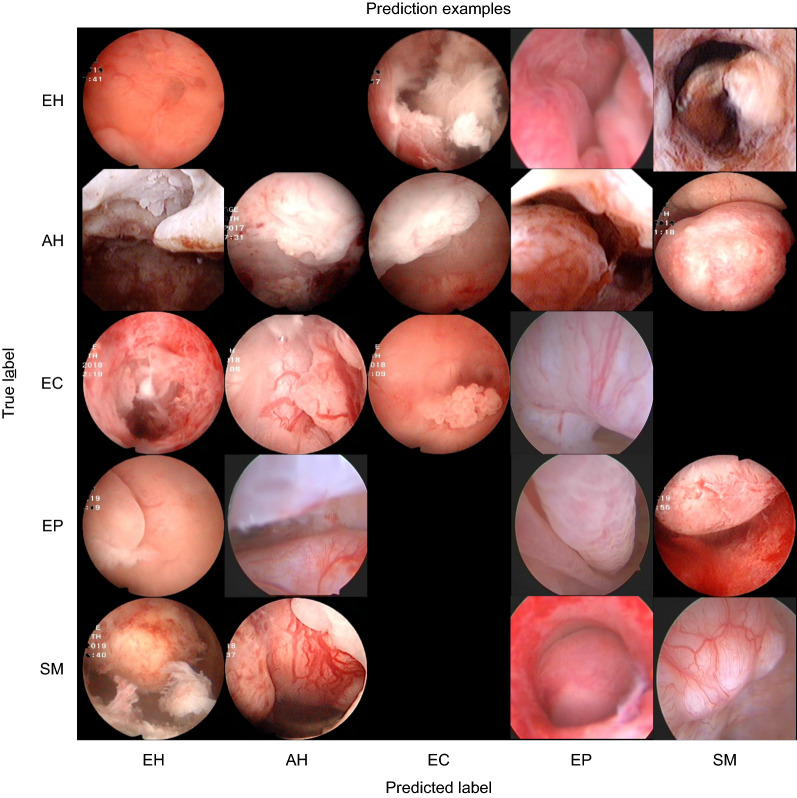
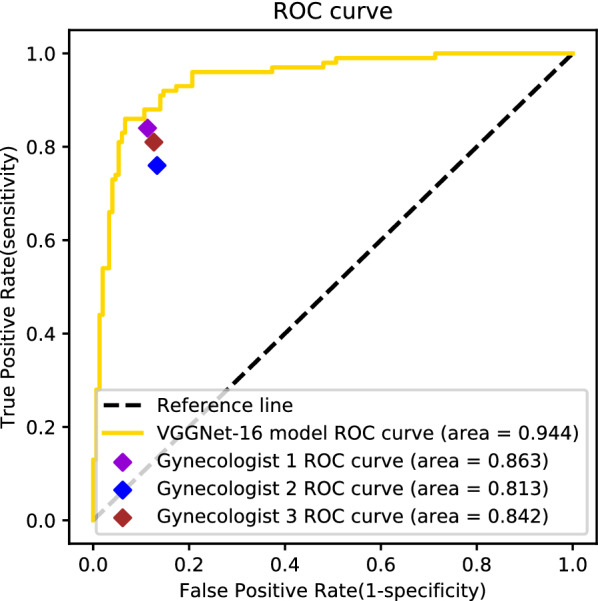
Results: The overall accuracy of the VGGNet-16 model in classifying endometrial lesions is 80.8%. Its sensitivity to endometrial hyperplasia without atypia, atypical hyperplasia, endometrial cancer, endometrial polyp, and submucous myoma is 84.0%, 68.0%, 78.0%, 94.0%, and 80.0%, respectively; for these diagnoses, the model's specificity is 92.5%, 95.5%, 96.5%, 95.0%, and 96.5%, respectively. When classifying lesions as benign or as premalignant/malignant, the VGGNet-16 model's accuracy, sensitivity, and specificity are 90.8%, 83.0%, and 96.0%, respectively. The diagnostic performance of the VGGNet-16 model is slightly better than that of the three gynecologists in both classification tasks. With the aid of the model, the overall accuracy of the diagnosis of endometrial lesions by gynecologists can be improved.
Conclusions: The VGGNet-16 model performs well in classifying endometrial lesions from hysteroscopic images and can provide objective diagnostic evidence for hysteroscopists.
Keywords: Computer-aided diagnosis; Convolutional neural network; Endometrial lesion; Hysteroscopy; VGGNet.
Conflict of interest statement
The author declares that they have no competing interests.
Figures
Similar articles
-
Hysteroscopic Photodynamic Diagnosis Using 5-Aminolevulinic Acid: A High-Sensitivity Diagnostic Method for Uterine Endometrial Malignant Diseases.J Minim Invasive Gynecol. 2020 Jul-Aug;27(5):1087-1094. doi: 10.1016/j.jmig.2019.08.012. Epub 2019 Aug 12. J Minim Invasive Gynecol. 2020. PMID: 31415818 Clinical Trial.
-
Automated system for diagnosing endometrial cancer by adopting deep-learning technology in hysteroscopy.PLoS One. 2021 Mar 31;16(3):e0248526. doi: 10.1371/journal.pone.0248526. eCollection 2021. PLoS One. 2021. PMID: 33788887 Free PMC article.
-
Hysteroscopy in women with abnormal uterine bleeding: a meta-analysis on four major endometrial pathologies.Arch Gynecol Obstet. 2015 Jun;291(6):1347-54. doi: 10.1007/s00404-014-3585-x. Epub 2014 Dec 19. Arch Gynecol Obstet. 2015. PMID: 25524536
-
Endometrial polyps. An evidence-based diagnosis and management guide.Eur J Obstet Gynecol Reprod Biol. 2021 May;260:70-77. doi: 10.1016/j.ejogrb.2021.03.017. Epub 2021 Mar 13. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 33756339 Review.
-
Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities.Cochrane Database Syst Rev. 2018 Dec 5;12(12):CD009461. doi: 10.1002/14651858.CD009461.pub4. Cochrane Database Syst Rev. 2018. PMID: 30521679 Free PMC article.
Cited by
-
Impact of artificial intelligence on the diagnosis, treatment and prognosis of endometrial cancer.Ann Med Surg (Lond). 2024 Jan 17;86(3):1531-1539. doi: 10.1097/MS9.0000000000001733. eCollection 2024 Mar. Ann Med Surg (Lond). 2024. PMID: 38463097 Free PMC article. Review.
-
Development of an Automated Morphometric Approach to Assess Vascular Outcomes following Exposure to Environmental Chemicals in Zebrafish.Environ Health Perspect. 2024 May;132(5):57001. doi: 10.1289/EHP13214. Epub 2024 May 3. Environ Health Perspect. 2024. PMID: 38701112 Free PMC article.
-
Unassisted Clinicians Versus Deep Learning-Assisted Clinicians in Image-Based Cancer Diagnostics: Systematic Review With Meta-analysis.J Med Internet Res. 2023 Mar 2;25:e43832. doi: 10.2196/43832. J Med Internet Res. 2023. PMID: 36862499 Free PMC article.
-
Demystifying Supervised Learning in Healthcare 4.0: A New Reality of Transforming Diagnostic Medicine.Diagnostics (Basel). 2022 Oct 20;12(10):2549. doi: 10.3390/diagnostics12102549. Diagnostics (Basel). 2022. PMID: 36292238 Free PMC article. Review.
-
Development of MRI-based radiomics predictive model for classifying endometrial lesions.Sci Rep. 2023 Jan 28;13(1):1590. doi: 10.1038/s41598-023-28819-2. Sci Rep. 2023. PMID: 36709399 Free PMC article.
References
-
- Cooper NA, Barton PM, Breijer M, Caffrey O, Opmeer BC, Timmermans A, Mol BW, Khan KS, Clark TJ. Cost-effectiveness of diagnostic strategies for the management of abnormal uterine bleeding (heavy menstrual bleeding and post-menopausal bleeding): a decision analysis. Health technology assessment (Winchester, England). 2014, 18(24):1–201, v–vi. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
