

Systematic early versus late mobilization or standard early mobilization in mechanically ventilated adult ICU patients: systematic review and meta-analysis
- PMID: 33407707
- PMCID: PMC7789482
- DOI: 10.1186/s13054-020-03446-9
Systematic early versus late mobilization or standard early mobilization in mechanically ventilated adult ICU patients: systematic review and meta-analysis
Abstract
Background: This systematic review and meta-analysis aimed to determine the effectiveness of systematic early mobilization in improving muscle strength and physical function in mechanically ventilated intensive care unit (ICU) patients.
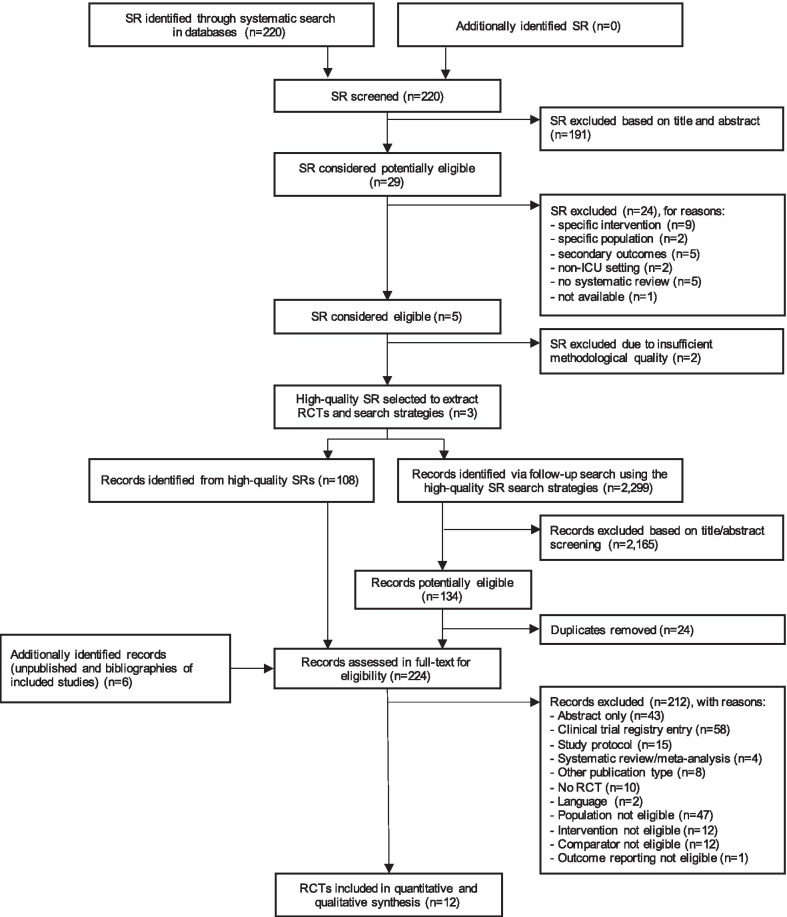
Methods: We conducted a two-stage systematic literature search in MEDLINE, EMBASE and the Cochrane Library until January 2019 for randomized controlled trials (RCTs) examining the effects of early mobilization initiated within 7 days after ICU admission compared with late mobilization, standard early mobilization or no mobilization. Priority outcomes were Medical Research Council Sum Score (MRC-SS), incidence of ICU-acquired weakness (ICUAW), 6-min walk test (6MWT), proportion of patients reaching independence, time needed until walking, SF-36 Physical Function Domain Score (PFS) and SF-36 Physical Health Component Score (PCS). Meta-analysis was conducted where sufficient comparable evidence was available. We evaluated the certainty of evidence according to the GRADE approach.
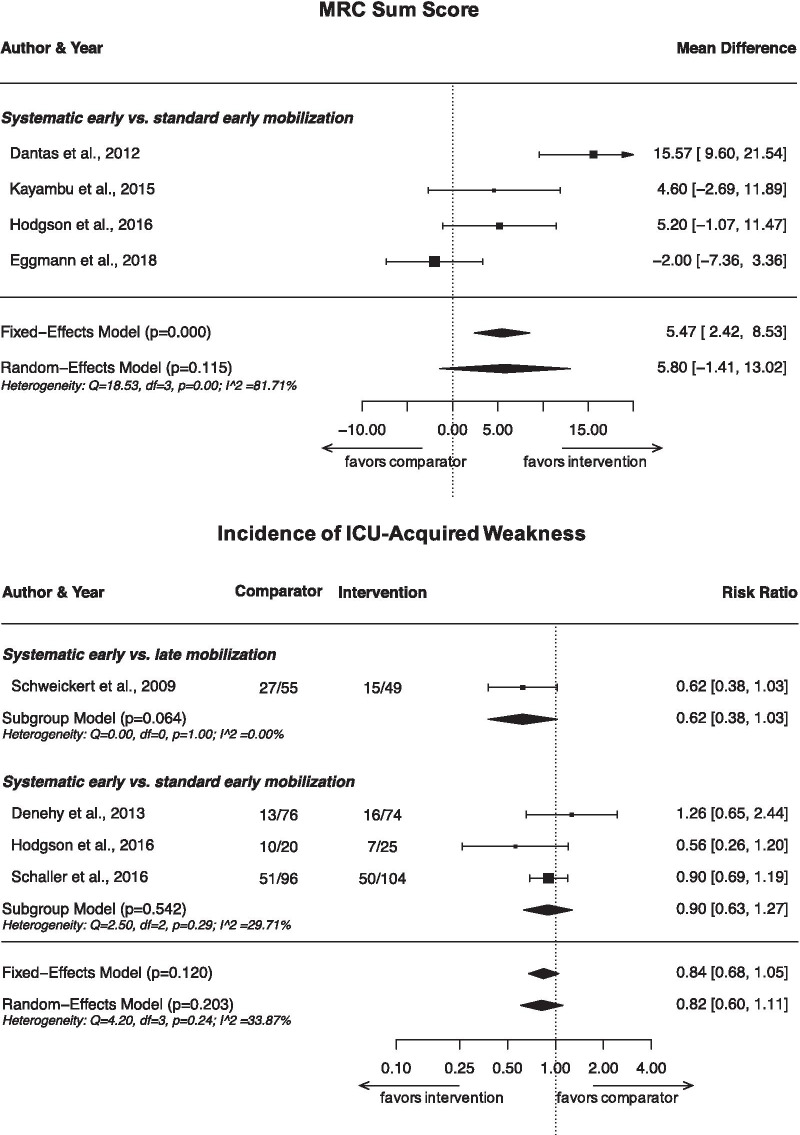
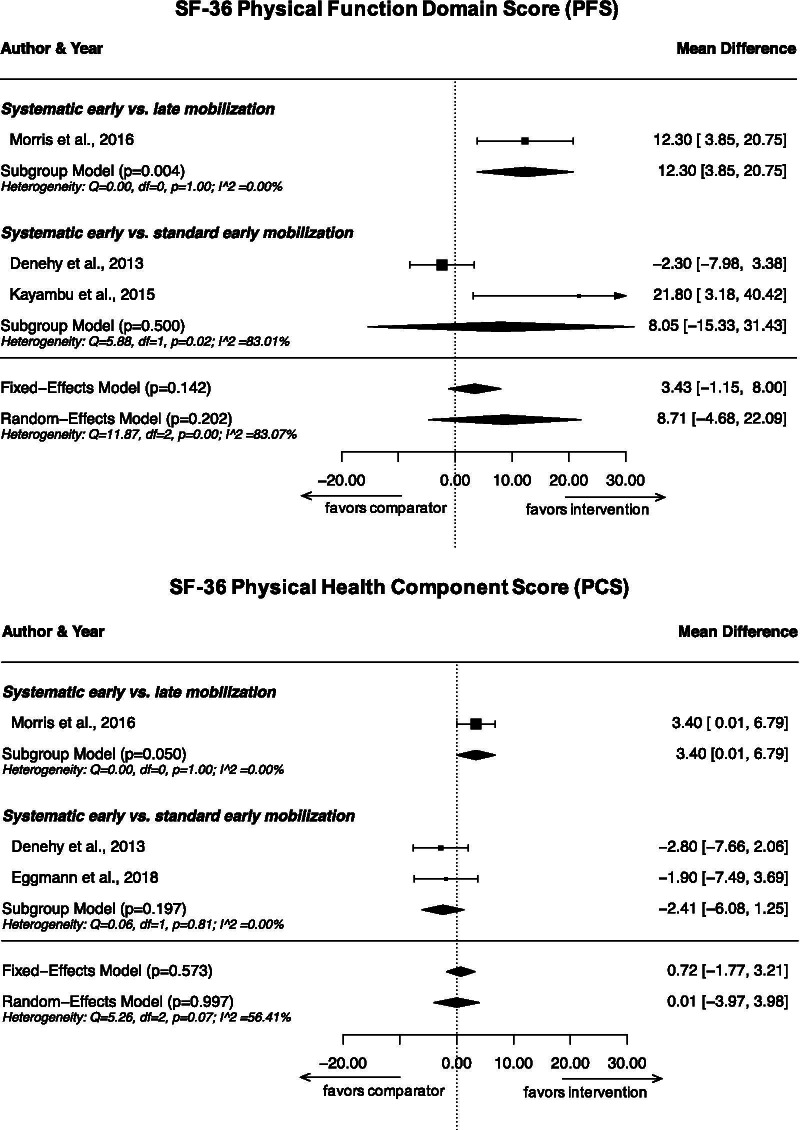
Results: We identified 12 eligible RCTs contributing data from 1304 participants. Two RCTs were categorized as comparing systematic early with late mobilization, nine with standard early mobilization and one with no mobilization. We found evidence for a benefit of systematic early mobilization compared to late mobilization for SF-36 PFS (MD 12.3; 95% CI 3.9-20.8) and PCS (MD 3.4; 95% CI 0.01-6.8), as well as on the proportion of patients reaching independence and the time needed to walking, but not for incidence of ICUAW (RR 0.62; 95% CI 0.38-1.03) or MRC-SS. For systematic early compared to standard early mobilization, we found no statistically significant benefit on MRC-SS (MD 5.8; 95% CI - 1.4 to 13.0), incidence of ICUAW (RR 0.90; 95% CI 0.63-1.27), SF-36 PFS (MD 8.1; 95% CI - 15.3 to 31.4) or PCS (MD - 2.4; 95% CI - 6.1 to 1.3) or other priority outcomes except for change in 6MWT from baseline. Generally, effects appeared stronger for systematic early compared to late mobilization than to standard early mobilization. We judged the certainty of evidence for all outcomes as very low to low.
Conclusion: The evidence regarding a benefit of systematic early mobilization remained inconclusive. However, our findings indicate that the larger the difference in the timing between the intervention and the comparator, the more likely an RCT is to find a benefit for early mobilization.
Study registration: PROSPERO (CRD42019122555).
Keywords: Critical care; Early mobilization; ICU; Intensive care; Mechanical ventilation; Meta-analysis; Physical therapy; Rehabilitation; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
