

Current challenges and controversies in the management of scapular fractures: a review
- PMID: 33407725
- PMCID: PMC7789406
- DOI: 10.1186/s13037-020-00281-3
Current challenges and controversies in the management of scapular fractures: a review
Abstract
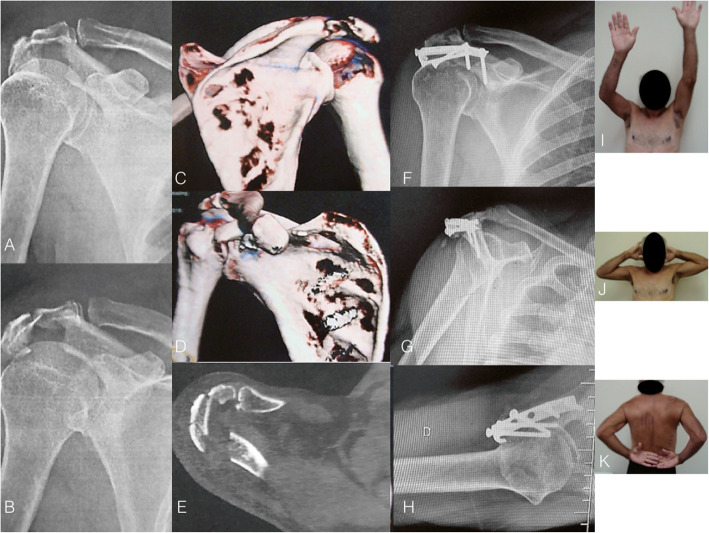
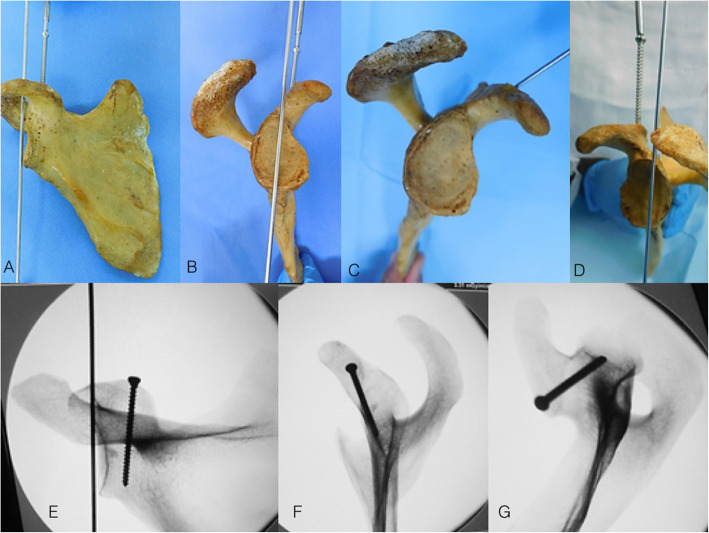
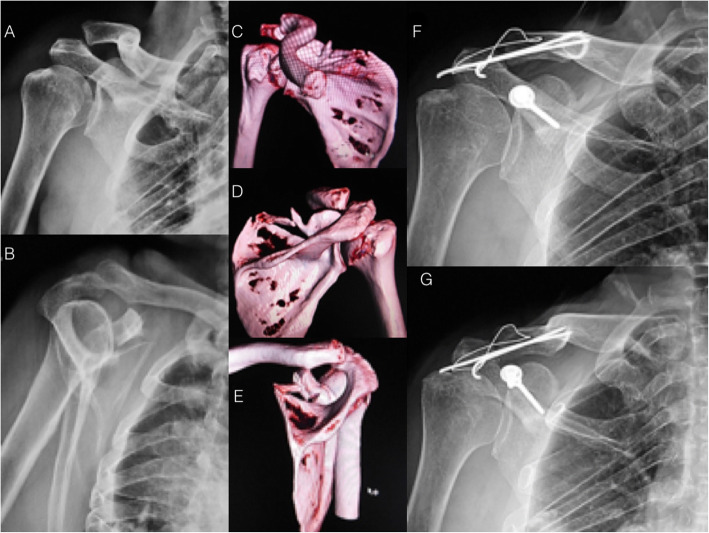
Fractures of the scapula are rare and usually associated with high-energy trauma. The unfavorable scapular anatomy, combined with the complexity of the approaches for fracture fixation, make the treatment challenging, even for experienced surgeons. Furthermore, the literature is controversial regarding surgical indications and rationale for treatment. The present review article was designed to address and discuss critical aspects of decision-making for the management of scapular fractures, including surgical indications and patient safety considerations.
Keywords: Complications; Floating shoulder; Non-operative treatment; Patient safety; Scapular fractures; Surgical decision-making.
Conflict of interest statement
The authors declare that they have no competing interests related with this article.
Figures
References
-
- Voleti P, Namdari S, Mehta S. Fractures of the scapula: diagnosis, indications, and operative technique. Univ Penn Orthop J. 2013;23:57–61.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
