

Mechanical power during extracorporeal membrane oxygenation and hospital mortality in patients with acute respiratory distress syndrome
- PMID: 33407733
- PMCID: PMC7787230
- DOI: 10.1186/s13054-020-03428-x
Mechanical power during extracorporeal membrane oxygenation and hospital mortality in patients with acute respiratory distress syndrome
Abstract
Background: Mechanical power (MP) refers to the energy delivered by a ventilator to the respiratory system per unit of time. MP referenced to predicted body weight (PBW) or respiratory system compliance have better predictive value for mortality than MP alone in acute respiratory distress syndrome (ARDS). Our objective was to assess the potential impact of consecutive changes of MP on hospital mortality among ARDS patients receiving extracorporeal membrane oxygenation (ECMO).
Methods: We performed a retrospective analysis of patients with severe ARDS receiving ECMO in a tertiary care referral center in Taiwan between May 2006 and October 2015. Serial changes of MP during ECMO were recorded.
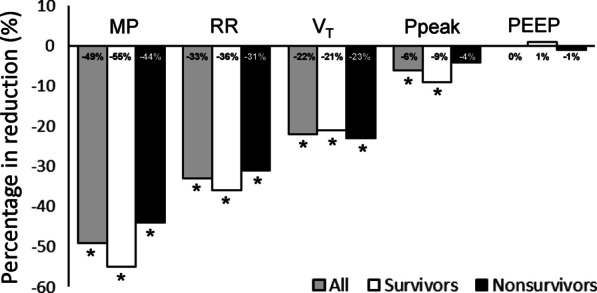
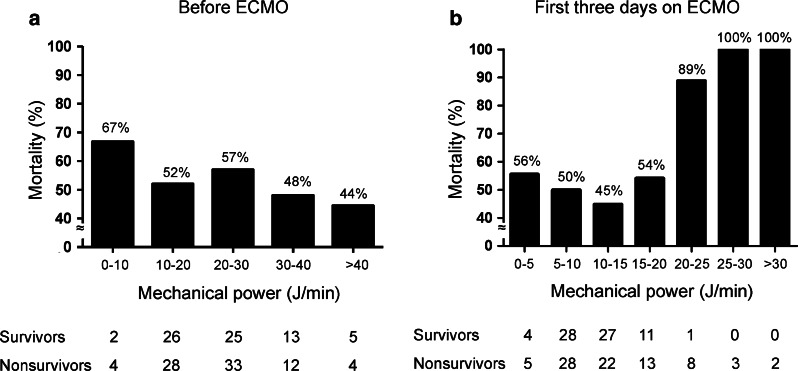
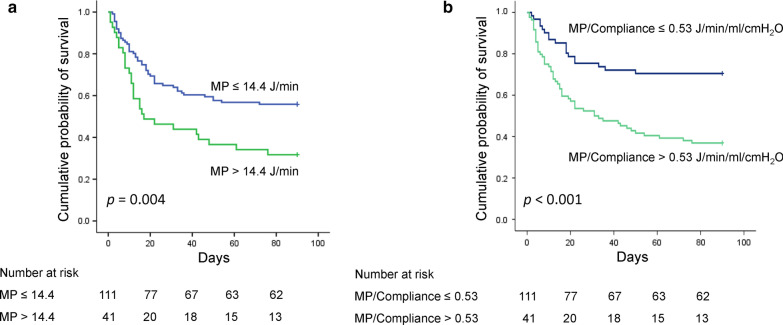
Results: A total of 152 patients with severe ARDS rescued with ECMO were analyzed. Overall hospital mortality was 53.3%. There were no significant differences between survivors and nonsurvivors in terms of baseline values of MP or other ventilator settings. Cox regression models demonstrated that mean MP alone, MP referenced to PBW, and MP referenced to compliance during the first 3 days of ECMO were all independently associated with hospital mortality. Higher MP referenced to compliance (HR 2.289 [95% CI 1.214-4.314], p = 0.010) was associated with a higher risk of death than MP itself (HR 1.060 [95% CI 1.018-1.104], p = 0.005) or MP referenced to PBW (HR 1.004 [95% CI 1.002-1.007], p < 0.001). The 90-day hospital mortality of patients with high MP (> 14.4 J/min) during the first 3 days of ECMO was significantly higher than that of patients with low MP (≦ 14.4 J/min) (70.7% vs. 46.8%, p = 0.004), and the 90-day hospital mortality of patients with high MP referenced to compliance (> 0.53 J/min/ml/cm H2O) during the first 3 days of ECMO was significantly higher than that of patients with low MP referenced to compliance (≦ 0.53 J/min/ml/cm H2O) (63.6% vs. 29.7%, p < 0.001).
Conclusions: MP during the first 3 days of ECMO was the only ventilatory variable independently associated with 90-day hospital mortality, and MP referenced to compliance during ECMO was more predictive for mortality than was MP alone.
Keywords: Acute respiratory distress syndrome; Compliance; Extracorporeal membrane oxygenation; Functional lung size; Mechanical power; Mortality; Ventilator-induced lung injury.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
