

A randomized trial of albumin infusion to prevent intradialytic hypotension in hospitalized hypoalbuminemic patients
- PMID: 33407747
- PMCID: PMC7789619
- DOI: 10.1186/s13054-020-03441-0
A randomized trial of albumin infusion to prevent intradialytic hypotension in hospitalized hypoalbuminemic patients
Abstract
Background: Intradialytic hypotension (IDH) is a frequent complication of intermittent hemodialysis (IHD), occurring from 15 to 50% of ambulatory sessions, and is more frequent among hospitalized patients with hypoalbuminemia. IDH limits adequate fluid removal and increases the risk for vascular access thrombosis, early hemodialysis (HD) termination, and mortality. Albumin infusion before and during therapy has been used for treating IDH with the varying results. We evaluated the efficacy of albumin infusion in preventing IDH during IHD in hypoalbuminemic inpatients.
Methods: A randomized, crossover trial was performed in 65 AKI or ESKD patients with hypoalbuminemia (albumin < 3 g/dl) who required HD during hospitalization. Patients were randomized to receive 100 ml of either 0.9%sodium chloride or 25% albumin intravenously at the initiation of each dialysis. These two solutions were alternated for up to six sessions. Patients' vital signs and ultrafiltration removal rate were recorded every 15 to 30 min during dialysis. IDH was assessed by different definitions reported in the literature. All symptoms associated with a noted hypotensive event as well as interventions during the dialysis were recorded.
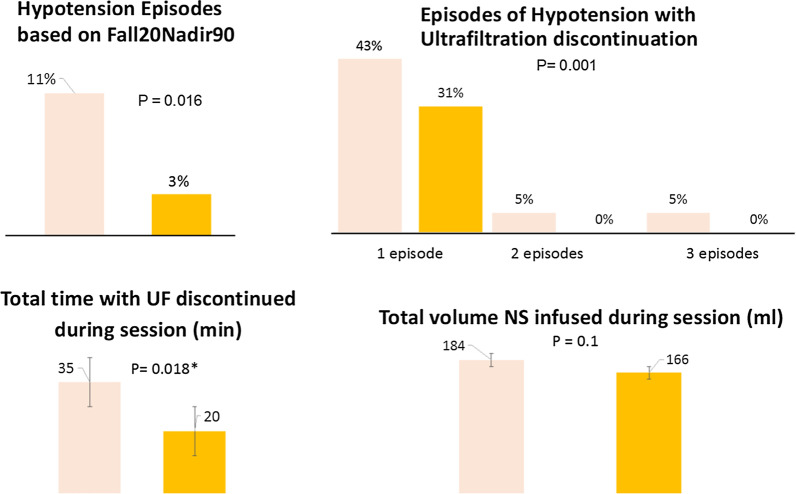
Results: Sixty-five patients were submitted to 249 sessions; the mean age was 58 ([Formula: see text] 12), and 46 (70%) were male with a mean weight of 76 ([Formula: see text] 18) kg. The presence of IDH was lower during albumin sessions based on all definitions. The hypotension risk was significantly decreased based on the Kidney Disease Outcomes Quality Initiative definition; (15% with NS vs. 7% with albumin, p = 0.002). The lowest intradialytic SBP was significantly worse in patients who received 0.9% sodium chloride than albumin (NS 83 vs. albumin 90 mmHg, p = 0.035). Overall ultrafiltration rate was significantly higher in the albumin therapies [NS - 8.25 ml/kg/h (- 11.18 5.80) vs. 8.27 ml/kg/h (- 12.22 to 5.53) with albumin, p = 0.011].
Conclusion: In hypoalbuminemic patients who need HD, albumin administration before the dialysis results in fewer episodes of hypotension and improves fluid removal. Albumin infusion may be of benefit to improve the safety of HD and achievement of fluid balance in these high-risk patients. ClinicalTrials.gov Identifier: NCT04522635.
Keywords: Acute kidney injury; Albumin; Chronic dialysis; Dialysis; Intradialytic hypotension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Kora M, Tawfeek A, El-Zorkany K, AbdEl-Mohsen A. The relationship between hypoalbuminemia and intradialytic hypotension in haemodialysis patients. J Kidney. 2018;4(1):110.
-
- Bouchard J, Soroko SB, Chertow GM, Himmelfarb J, Ikizler TA, Paganini EP, et al. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009;76(4):422–427. - PubMed
-
- Berthelsen RE, Perner A, Jensen AK, Rasmussen BS, Jensen JU, Wiis J, et al. Forced fluid removal in intensive care patients with acute kidney injury: the randomised FFAKI feasibility trial. Acta Anaesthesiol Scand. 2018;62(7):936–944. - PubMed
-
- Moore PK, Hsu RK, Liu KD. Management of acute kidney injury: core curriculum 2018. Am J Kidney Dis. 2018;72(1):136–148. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
