

Prehospital identification of Covid-19: an observational study
- PMID: 33407750
- PMCID: PMC7786859
- DOI: 10.1186/s13049-020-00826-6
Prehospital identification of Covid-19: an observational study
Abstract
Background: The novel coronavirus disease 2019 (Covid-19) pandemic has affected prehospital care systems across the world, but the prehospital presentation of affected patients and the extent to which prehospital care providers are able to identify them is not well characterized. In this study, we describe the presentation of Covid-19 patients in a Swedish prehospital care system, and asses the predictive value of Covid-19 suspicion as documented by dispatch and ambulance nurses.
Methods: Data for all patients with dispatch, ambulance, and hospital records between January 1-August 31, 2020 were extracted. A descriptive statistical analysis of patients with and without hospital-confirmed Covid-19 was performed. In a subset of records beginning from April 14, we assessed the sensitivity and specificity of documented Covid-19 suspicion in dispatch and ambulance patient care records.
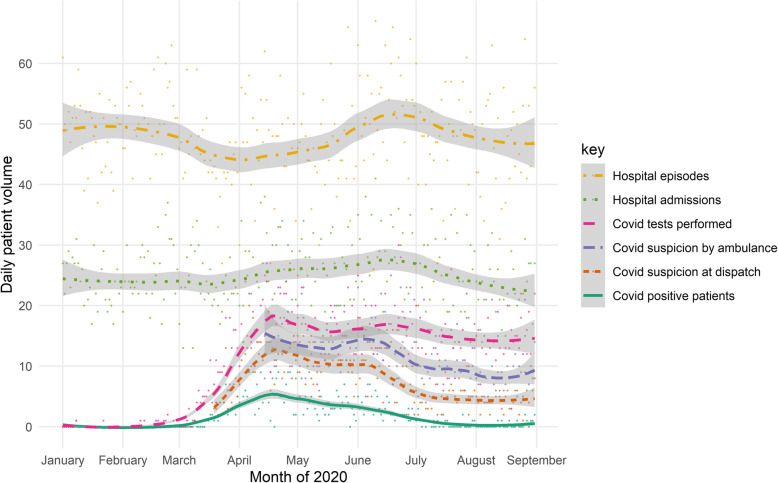
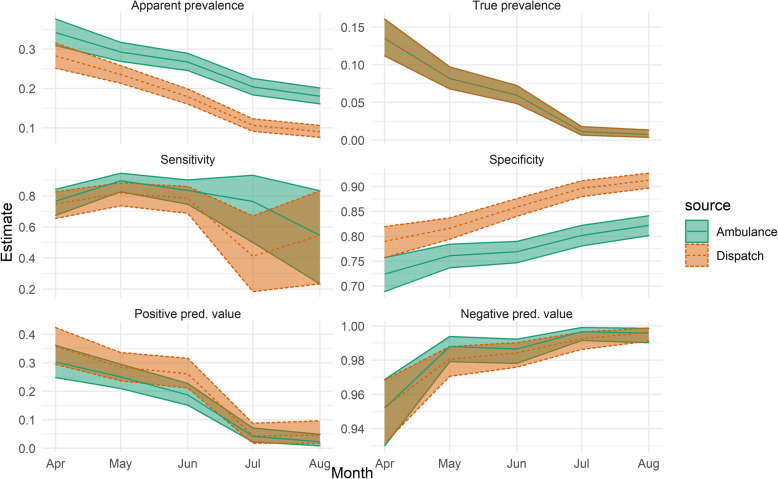
Results: A total of 11,894 prehospital records were included, of which 481 had a primary hospital diagnosis code related to-, or positive test results for Covid-19. Covid-19-positive patients had considerably worse outcomes than patients with negative test results, with 30-day mortality rates of 24% vs 11%, but lower levels of prehospital acuity (e.g. emergent transport rates of 14% vs 22%). About half (46%) of Covid-19-positive patients presented to dispatchers with primary complaints typically associated with Covid-19. Six thousand seven hundred seventy-six records were included in the assessment of predictive value. Sensitivity was 76% (95% CI 71-80) and 82% (78-86) for dispatch and ambulance suspicion respectively, while specificities were 86% (85-87) and 78% (77-79).
Conclusions: While prehospital suspicion was strongly indicative of hospital-confirmed Covid-19, based on the sensitivity identified in this study, prehospital suspicion should not be relied upon as a single factor to rule out the need for isolation precautions. The data provided may be used to develop improved guidelines for identifying Covid-19 patients in the prehospital setting.
Conflict of interest statement
The authors are employed by the regional ambulance service studied. The authors declare that they have no further competing interests.
Figures


References
-
- Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, et al. Clinical, laboratory and imaging features of COVID-19: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;34:101623. doi: 10.1016/j.tmaid.2020.101623. - DOI - PMC - PubMed
-
- Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi: 10.1016/S0140-6736(20)31142-9. - DOI - PMC - PubMed
-
- Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;323(18):1824–1836. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
