

Characteristics and clinical outcomes of culture-negative and culture-positive septic shock: a single-center retrospective cohort study
- PMID: 33407768
- PMCID: PMC7787242
- DOI: 10.1186/s13054-020-03421-4
Characteristics and clinical outcomes of culture-negative and culture-positive septic shock: a single-center retrospective cohort study
Abstract
Background: We evaluated the characteristics and outcomes of culture-negative versus culture-positive septic shock.
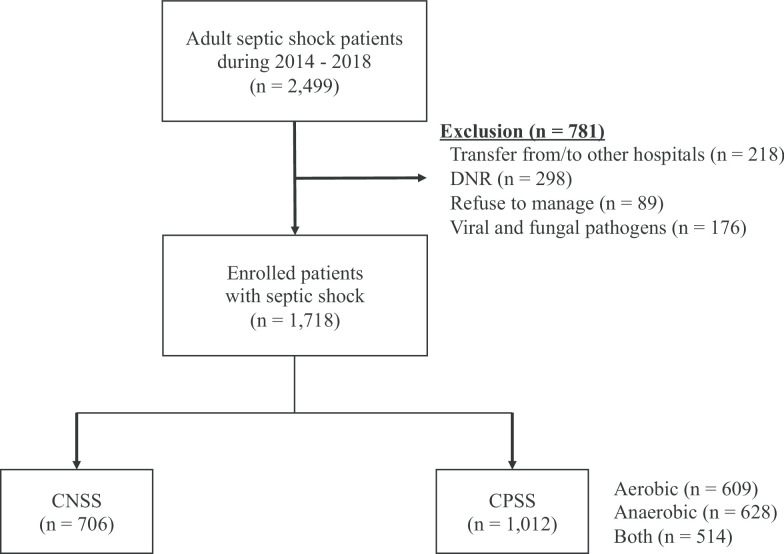
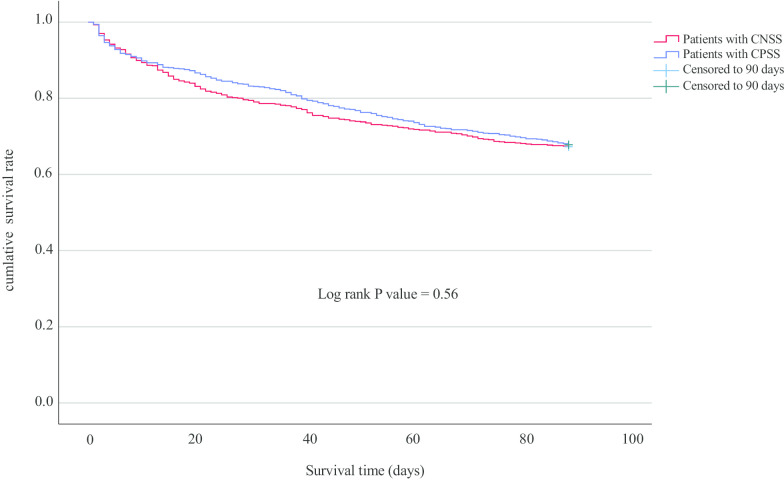
Methods: We performed a retrospective observational study of data from a prospective registry from 2014 to 2018. A total of 2,499 adult patients with septic shock were enrolled. The primary outcome was 90-day mortality, and the secondary outcomes were the length of hospital stay, a requirement for mechanical ventilation or renal replacement therapy, and in-hospital mortality.
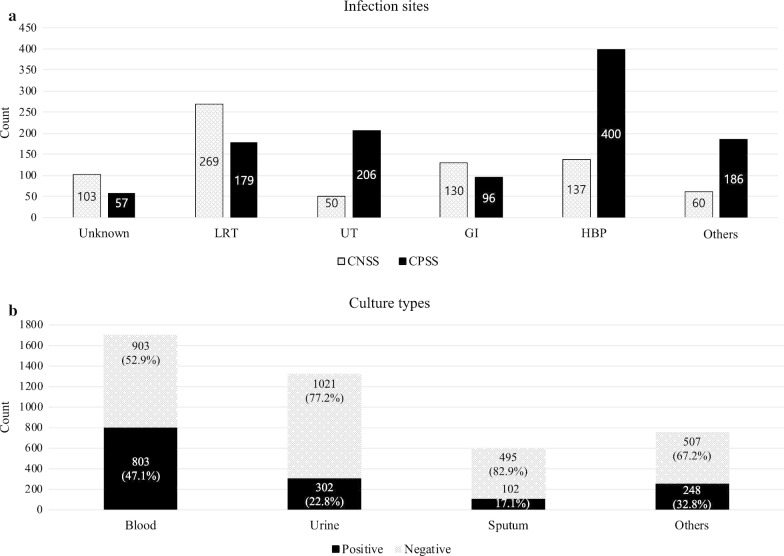
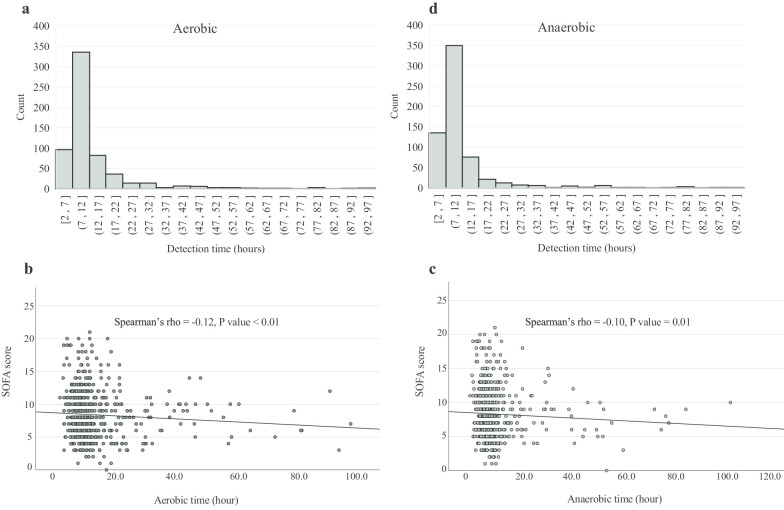
Results: Of 1,718 patients with septic shock, 1,012 (58.9%) patients were culture-positive (blood 803, urine 302, sputum 102, others 204) and the median pathogen detection time was 9.5 h (aerobic 10.2 h and anaerobic 9.0 h). The most common site of culture-positive infection was the hepatobiliary tract (39.5%), while for the culture-negative it was the lower respiratory tract (38.2%). The culture-negative group had a lower mean body temperature (37.3 vs 37.7 ℃), lactate (2.5 vs. 3.2 mmol/L), C-reactive protein (11.1 vs 11.9 mg/dL), and sequential organ failure assessment score (7.0 vs. 8.0) than that of the culture-positive group. However, 90-day mortality between the groups was not significantly different (32.7 vs 32.2%, p = 0.83), and the other clinical outcomes also did not differ significantly. Moreover, a shorter culture detection time was correlated with a higher sequential organ failure assessment score but not with mortality.
Conclusion: Patients with septic shock are frequently culture-negative, especially in cases where the infection focus is in the lower respiratory tract. Although culture-negative was associated with a degree of organ dysfunction, it was not an independent predictor of death.
Keywords: Culture; Mortality; Sepsis; Septic shock; Time to blood culture positivity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
