

Characteristics and outcomes of patients admitted to adult intensive care units in Hong Kong: a population retrospective cohort study from 2008 to 2018
- PMID: 33407925
- PMCID: PMC7788755
- DOI: 10.1186/s40560-020-00513-9
Characteristics and outcomes of patients admitted to adult intensive care units in Hong Kong: a population retrospective cohort study from 2008 to 2018
Abstract
Background: Globally, mortality rates of patients admitted to the intensive care unit (ICU) have decreased over the last two decades. However, evaluations of the temporal trends in the characteristics and outcomes of ICU patients in Asia are limited. The objective of this study was to describe the characteristics and risk adjusted outcomes of all patients admitted to publicly funded ICUs in Hong Kong over a 11-year period. The secondary objective was to validate the predictive performance of Acute Physiology And Chronic Health Evaluation (APACHE) IV for ICU patients in Hong Kong.
Methods: This was an 11-year population-based retrospective study of all patients admitted to adult general (mixed medical-surgical) intensive care units in Hong Kong public hospitals. ICU patients were identified from a population electronic health record database. Prospectively collected APACHE IV data and clinical outcomes were analysed.
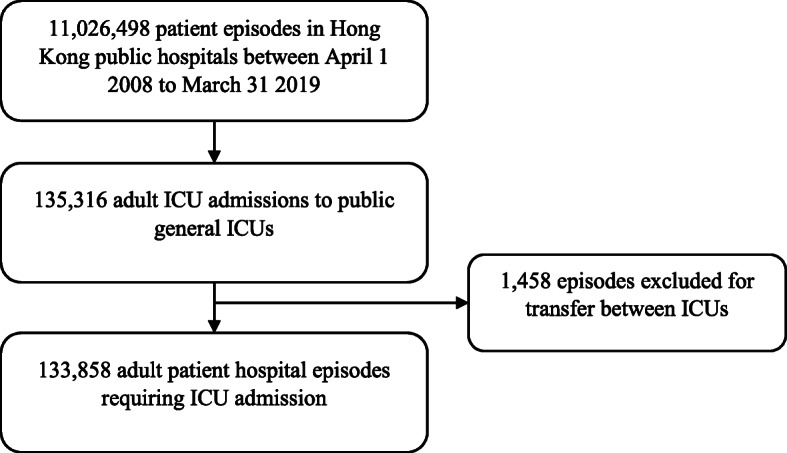
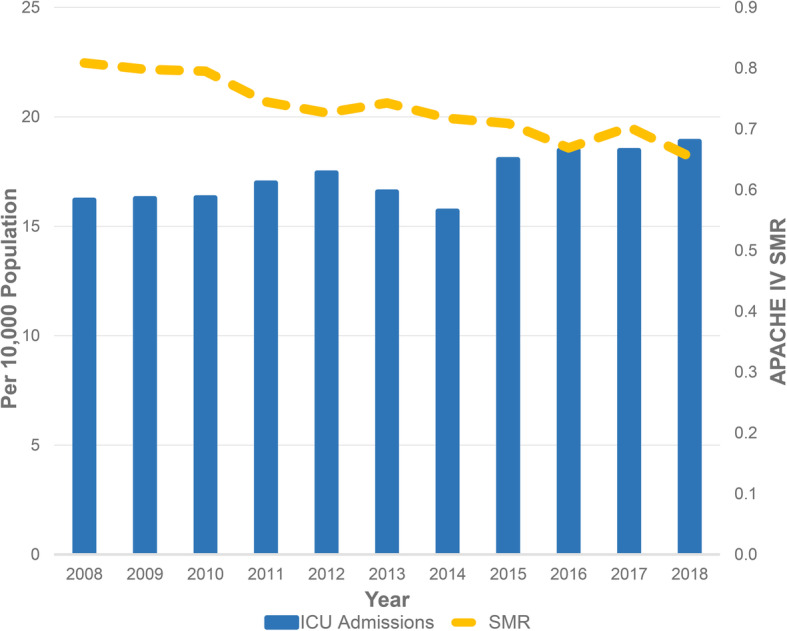
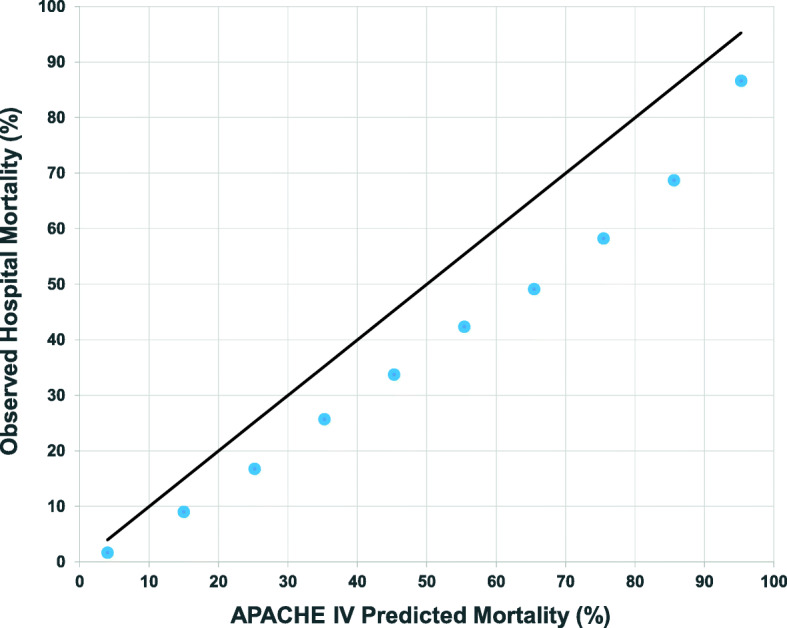
Results: From 1 April 2008 to 31 March 2019, there were a total of 133,858 adult ICU admissions in Hong Kong public hospitals. During this time, annual ICU admissions increased from 11,267 to 14,068, whilst hospital mortality decreased from 19.7 to 14.3%. The APACHE IV standard mortality ratio (SMR) decreased from 0.81 to 0.65 during the same period. Linear regression demonstrated that APACHE IV SMR changed by - 0.15 (95% CI - 0.18 to - 0.11) per year (Pearson's R = - 0.951, p < 0.001). Observed median ICU length of stay was shorter than that predicted by APACHE IV (1.98 vs. 4.77, p < 0.001). C-statistic for APACHE IV to predict hospital mortality was 0.889 (95% CI 0.887 to 0.891) whilst calibration was limited (Hosmer-Lemeshow test p < 0.001).
Conclusions: Despite relatively modest per capita health expenditure, and a small number of ICU beds per population, Hong Kong consistently provides a high-quality and efficient ICU service. Number of adult ICU admissions has increased, whilst adjusted mortality has decreased over the last decade. Although APACHE IV had good discrimination for hospital mortality, it overestimated hospital mortality of critically ill patients in Hong Kong.
Keywords: APACHE IV; Benchmarking; Hong Kong; Intensive care; Standard mortality ratio.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Moran JL, Bristow P, Solomon PJ, George C, Hart GK, Australian, New Zealand Intensive Care Society Database Management C Mortality and length-of-stay outcomes, 1993-2003, in the binational Australian and New Zealand intensive care adult patient database. Crit Care Med. 2008;36(1):46–61. doi: 10.1097/01.CCM.0000295313.08084.58. - DOI - PubMed
-
- Olaechea PM, Alvarez-Lerma F, Palomar M, Gimeno R, Gracia MP, Mas N, Rivas R, Seijas I, Nuvials X, Catalan M, et al. Characteristics and outcomes of patients admitted to Spanish ICU: A prospective observational study from the ENVIN-HELICS registry (2006-2011) Med Intensiva. 2016;40(4):216–229. doi: 10.1016/j.medin.2015.07.003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
