

Cervicovaginal bacterial communities in reproductive-aged Tanzanian women with Schistosoma mansoni, Schistosoma haematobium, or without schistosome infection
- PMID: 33408370
- PMCID: PMC8115289
- DOI: 10.1038/s41396-020-00868-9
Cervicovaginal bacterial communities in reproductive-aged Tanzanian women with Schistosoma mansoni, Schistosoma haematobium, or without schistosome infection
Abstract
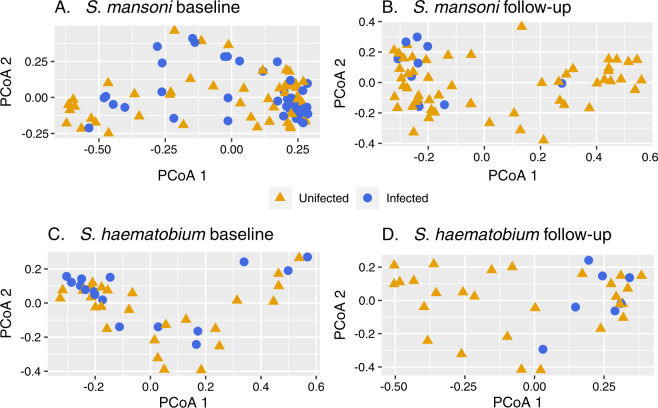
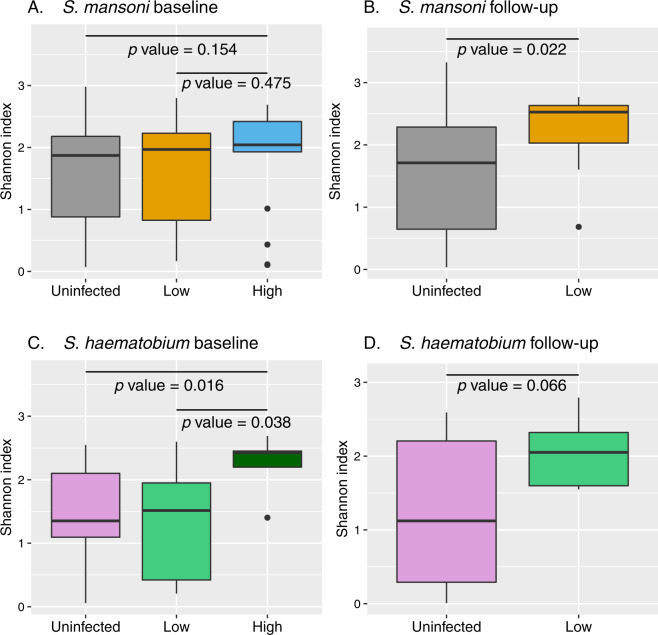
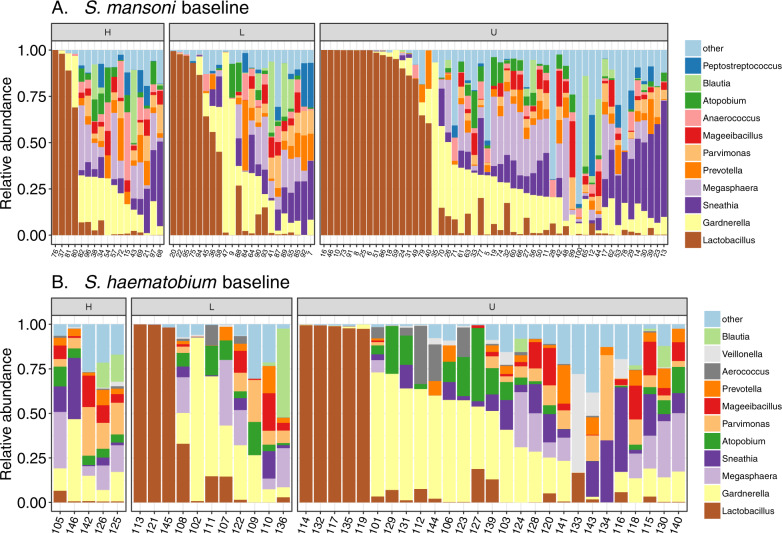
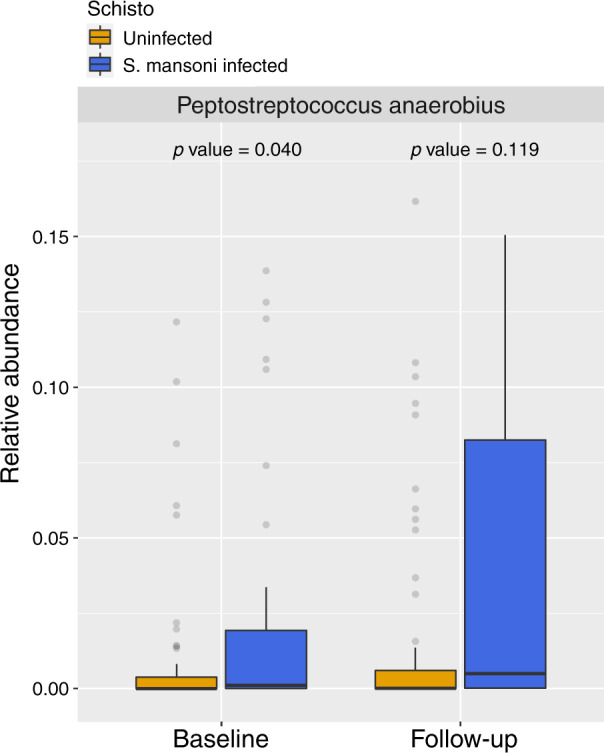
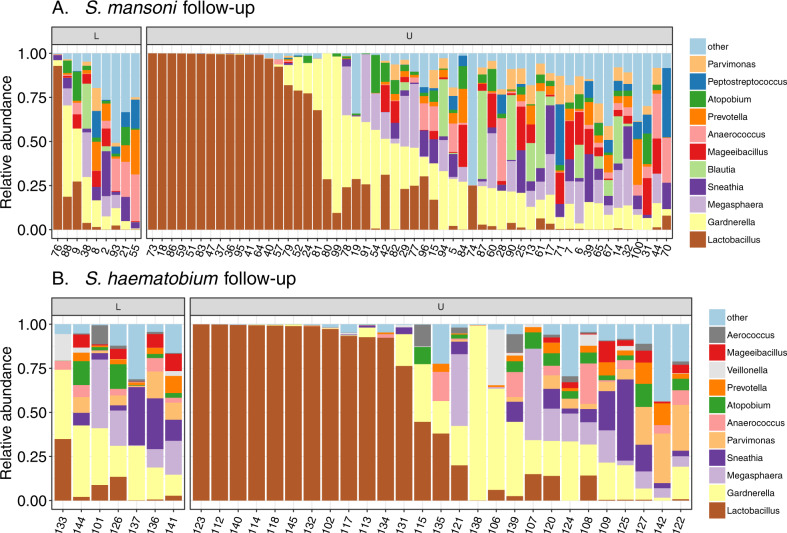
Schistosome infection is recognized as a potentially modifiable risk factor for HIV in women by the World Health Organization. Alterations in cervicovaginal bacteria have been associated with HIV acquisition and have not been studied in schistosome infection. We collected cervical swabs from Tanzanian women with and without S. mansoni and S. haematobium to determine effects on cervicovaginal microbiota. Infected women were treated, and follow-up swabs were collected after 3 months. 16S rRNA sequencing was performed on DNA extracted from swabs. We compared 39 women with S. mansoni with 52 uninfected controls, and 16 with S. haematobium with 27 controls. S. mansoni-infected women had increased abundance of Peptostreptococcus (p = 0.026) and presence of Prevotella timonesis (p = 0.048) compared to controls. High-intensity S. haematobium infection was associated with more diverse cervicovaginal bacterial communities than uninfected controls (p = 0.0159). High-intensity S. mansoni infection showed a similar trend (p = 0.154). At follow-up, we observed increased alpha diversity in S. mansoni (2.53 vs. 1.72, p = 0.022) and S. haematobium (2.05 vs. 1.12, p = 0.066) infection groups compared to controls. Modifications in cervicovaginal microbiota, particularly increased diversity and abundance of taxa associated with bacterial vaginosis and HIV (Peptostreptococcus, Prevotella), were associated with schistosome infection.
Keywords: Cervicovaginal microbiota; HIV; Microbiome; Schistosomiasis; Tanzania.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Kjetland EF, Ndhlovu PD, Gomo E, Mduluza T, Midzi N, Gwanzura L, et al. Association between genital schistosomiasis and HIV in rural Zimbabwean women. AIDS. 2006;20:593–600. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
