

Sixty-Day Mortality Among 520 Italian Hospitalized COVID-19 Patients According to the Adopted Ventilatory Strategy in the Context of an Integrated Multidisciplinary Clinical Organization: A Population-Based Cohort Study
- PMID: 33408529
- PMCID: PMC7779307
- DOI: 10.2147/CLEP.S278709
Sixty-Day Mortality Among 520 Italian Hospitalized COVID-19 Patients According to the Adopted Ventilatory Strategy in the Context of an Integrated Multidisciplinary Clinical Organization: A Population-Based Cohort Study
Abstract
Purpose: Although the decision of which ventilation strategy to adopt in COVID-19 patients is crucial, yet the most appropriate means of carrying out this undertaking is not supported by strong evidence. We therefore described the organization of a province-level healthcare system during the occurrence of the COVID-19 epidemic and the 60-day outcomes of the hospitalized COVID-19 patients according to the respiratory strategy adopted given the limited available resources.
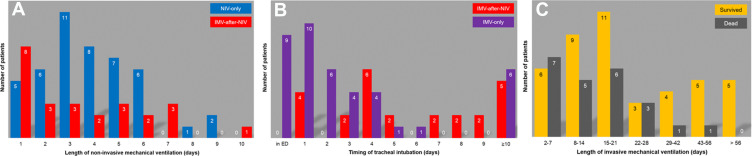
Patients and methods: All COVID-19 patients (26/02/2020-18/04/2020) in the Rimini Province of Italy were included in this population-based cohort study. The hospitalized patients were classified according to the maximum level of respiratory support: oxygen supplementation (Oxygen group), non-invasive ventilation (NIV-only group), invasive mechanical ventilation (IMV-only group), and IMV after an NIV trial (IMV-after-NIV group). Sixty-day mortality risk was estimated with a Cox proportional hazard analysis adjusted by age, sex, and administration of steroids, canakinumab, and tocilizumab.
Results: We identified a total of 1,424 symptomatic patients: 520 (36.5%) were hospitalized, while 904 (63.5%) were treated at home with no 60-day deaths. Based on the respiratory support, 408 (78.5%) were assigned to the Oxygen group, 46 (8.8%) to the NIV-only group, 25 (4.8%) to the IMV-after-NIV group, and 41 (7.9%) to the IMV-only group. There was no significant difference in the PaO2/FiO2 at IMV inception in the IMV-after-NIV and IMV-only groups (p=0.9). Overall 60-day mortality was 24.2% (Oxygen: 23.0%; NIV-only: 19.6%; IMV-after-NIV: 32.0%; IMV-only: 36.6%; p=0.165). Compared with the Oxygen group, the adjusted 60-day mortality risk significantly increased in the IMV-after-NIV (HR 2.776; p=0.024) and IMV-only groups (HR 2.966; p=0.001).
Conclusion: This study provided a population-based estimate of the impact of the COVID-19 outbreak in a severely affected Italian province. A similar 60-day mortality risk was found for patients undergoing immediate IMV and those intubated after an NIV trial with favorable outcomes after prolonged IMV.
Keywords: ARDS; COVID-19; mechanical ventilation; mortality; multidisciplinary team approach; noninvasive ventilation.
© 2020 Potalivo et al.
Conflict of interest statement
Jonathan Montomoli reports personal fees from Active Medical BV, outside the submitted work. The authors report no other potential conflicts of interest for this work.
Figures


References
-
- ICNARC. Intensive Care National Audit & Research Centre (ICNARC) report on COVID-19 in critical care - 17 July 2020. Available from: https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports. Accessed August24, 2020.
LinkOut - more resources
Full Text Sources
