

IDH1-mutant primary intraventricular gliosarcoma: Case report and systematic review of a rare location and molecular profile
- PMID: 33408906
- PMCID: PMC7771479
- DOI: 10.25259/SNI_586_2020
IDH1-mutant primary intraventricular gliosarcoma: Case report and systematic review of a rare location and molecular profile
Abstract
Background: Gliosarcoma (GS) is classified as an IDH-wild-type variant of glioblastoma (GBM). While GS is already an unusual presentation of GBM, IDH1-mutant cases are especially rare. We present an IDH1-mutant primary intraventricular GS case report and a systematic review of the molecular profile in GS correlating to the prognostic and pathogenesis of IDH1/2 mutations.
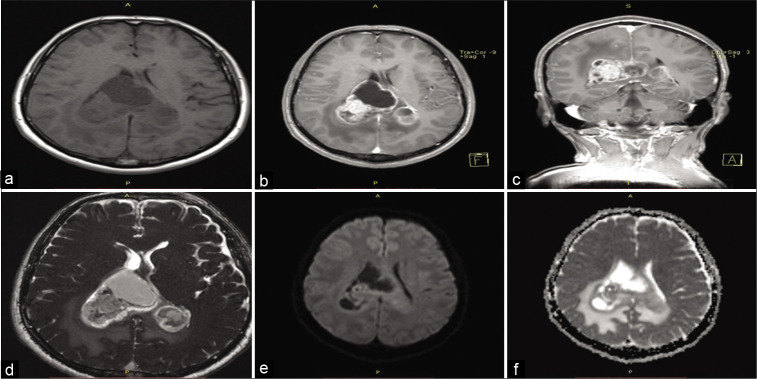
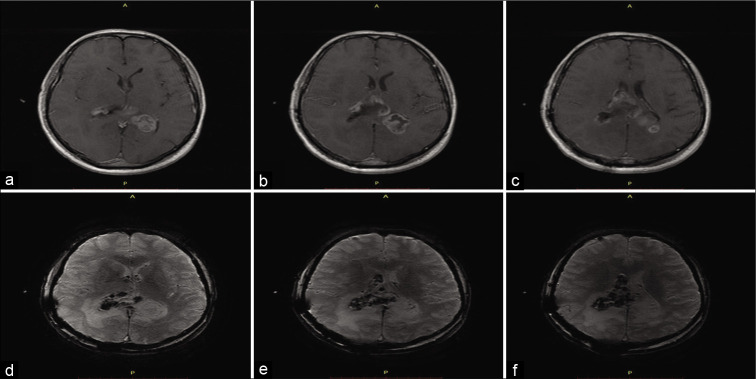
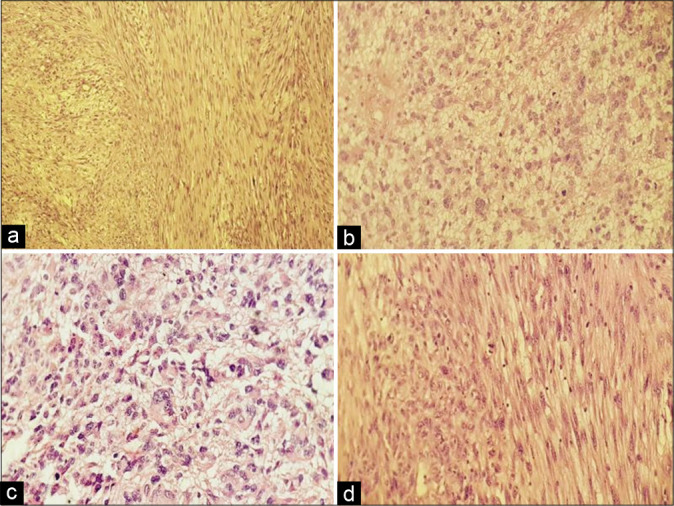
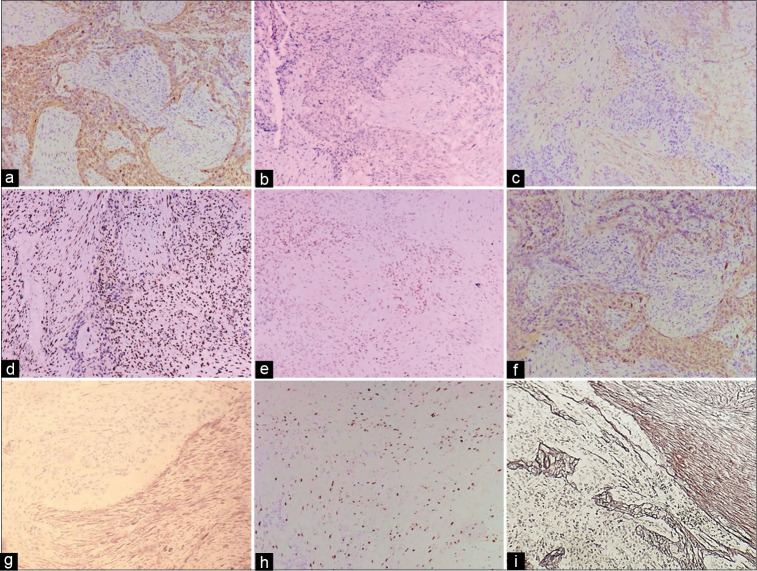
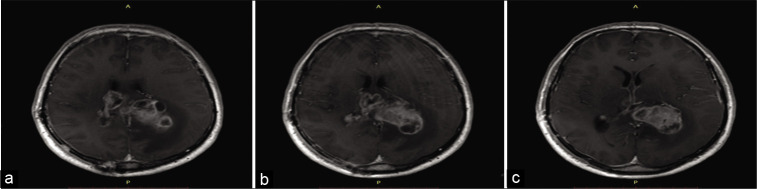
Case description: A 44-years-old man presented with ongoing fatigue symptoms and a new-onset intense occipital headache. The patient complained of memory loss, dyscalculia, and concentration difficulties. An MRI revealed a bihemispheric intraventricular mass crossing the midline through the corpus callosum and infiltrating the trigone of the lateral ventricles, hypointense, and hyperintense on the T1- and T2-weighted image. We performed a microsurgical resection with a transparietal transsulcal approach; however, the contralateral mass was attached to vascular structures and we decided to reoperate the patient in another moment. The histopathological study showed a Grade IV tumor and the immunohistochemistry confirmed the diagnosis of GS. The patient presented progressive neurologic decline and died 45 days after the surgical approach.
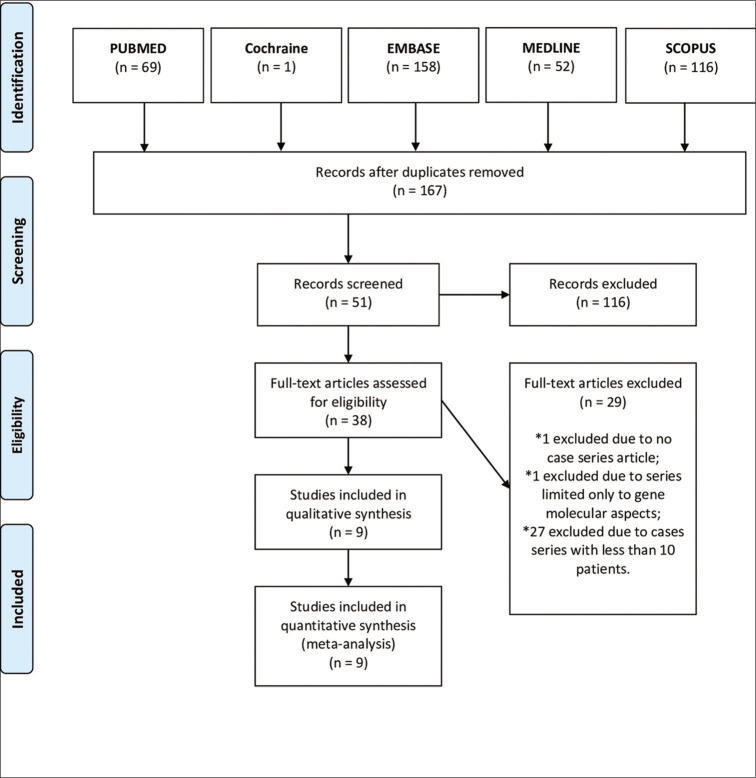
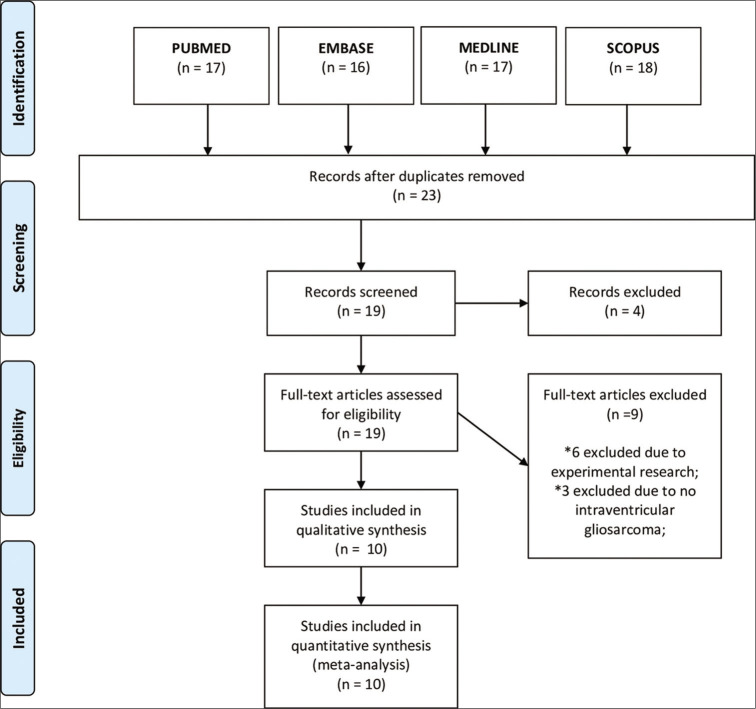
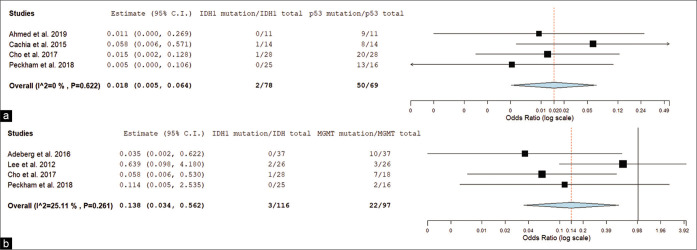
Conclusion: We did two systematic reviews studies from PubMed, EMBASE, MEDLINE, Cochrane, and SCOPUS databases, and included molecular and intraventricular studies of GS. We performed further meta-analysis using OpenMetaAnalyst™ software. We conducted a forest plot with the molecular profile of GS. When correlated IDH1 mutation versus tp53 mutation, we found an odds ratio (OR) of 0.018 (0.005-0.064) and P < 0.001. Moreover, we compared IDH1 mutation versus MGMT methylation (P = 0.006; OR = 0.138 [0.034-0.562]). The studies evaluating the molecular profile in GS prognostics are often extended from all GBMs despite specifics GBM variants (i.e., GS). We found a correlation between IDH1 mutation expression with tp53 and MGMT expression in GS, and future studies exploring this molecular profile in GS are strongly encouraged.
Keywords: Case report; Cerebral ventricle neoplasms; Gliosarcoma; Human IDH1 protein; Systematic review.
Copyright: © 2020 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
A Rare Tumor in a Rare Location: Radiology and Pathology Findings With a Literature Review on Intraventricular Gliosarcoma.Cureus. 2023 Feb 4;15(2):e34622. doi: 10.7759/cureus.34622. eCollection 2023 Feb. Cureus. 2023. PMID: 36891012 Free PMC article.
-
IDH1 mutations is prognostic marker for primary glioblastoma multiforme but MGMT hypermethylation is not prognostic for primary glioblastoma multiforme.Gene. 2015 Jan 1;554(1):81-6. doi: 10.1016/j.gene.2014.10.027. Epub 2014 Oct 14. Gene. 2015. PMID: 25455102
-
Gliosarcoma with osteosarcomatous component: A case report and short review illustration.Pathol Res Pract. 2022 Apr;232:153837. doi: 10.1016/j.prp.2022.153837. Epub 2022 Mar 7. Pathol Res Pract. 2022. PMID: 35278815
-
Glioblastoma: pathology, molecular mechanisms and markers.Acta Neuropathol. 2015 Jun;129(6):829-48. doi: 10.1007/s00401-015-1432-1. Epub 2015 May 6. Acta Neuropathol. 2015. PMID: 25943888 Review.
-
Primary Intracranial Gliosarcoma: Is It Really a Variant of Glioblastoma? An Update of the Clinical, Radiological, and Biomolecular Characteristics.J Clin Med. 2023 Dec 22;13(1):83. doi: 10.3390/jcm13010083. J Clin Med. 2023. PMID: 38202090 Free PMC article. Review.
Cited by
-
Computed Tomography, Magnetic Resonance Imaging, and Pathological Features of Gliosarcoma.Neuropsychiatr Dis Treat. 2022 Nov 4;18:2577-2589. doi: 10.2147/NDT.S386616. eCollection 2022. Neuropsychiatr Dis Treat. 2022. PMID: 36387942 Free PMC article.
-
A Rare Tumor in a Rare Location: Radiology and Pathology Findings With a Literature Review on Intraventricular Gliosarcoma.Cureus. 2023 Feb 4;15(2):e34622. doi: 10.7759/cureus.34622. eCollection 2023 Feb. Cureus. 2023. PMID: 36891012 Free PMC article.
-
Gliomas Infiltrating the Corpus Callosum: A Systematic Review of the Literature.Cancers (Basel). 2022 May 19;14(10):2507. doi: 10.3390/cancers14102507. Cancers (Basel). 2022. PMID: 35626112 Free PMC article. Review.
-
Sarcomatous transformation of IDH-mutant astrocytoma matching to methylation class oligosarcoma following embolization, a case report.Acta Neuropathol Commun. 2024 Dec 20;12(1):196. doi: 10.1186/s40478-024-01908-7. Acta Neuropathol Commun. 2024. PMID: 39707480 Free PMC article.
-
Primary intraventricular gliosarcoma on MRI: A challenging diagnosis.Radiol Case Rep. 2021 Dec 28;17(3):685-689. doi: 10.1016/j.radcr.2021.12.022. eCollection 2022 Mar. Radiol Case Rep. 2021. PMID: 35003460 Free PMC article.
References
-
- Adeberg S, Bernhardt D, Harrabi SB, Diehl C, Koelsche C, Rieken S, et al. Radiotherapy plus concomitant temozolomide in primary gliosarcoma. J Neurooncol. 2016;128:341–8. - PubMed
-
- Alkhaibary A, Alassiri AH, AlSufiani F, Alharbi MA. Ki-67 labeling index in glioblastoma; does it really matter? Hematol Oncol Stem Cell Ther. 2019;12:82–8. - PubMed
-
- Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, et al. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013;126:267–76. - PubMed
-
- Baldawa S, Kasegaonkar P, Vani S, Kelkar G. Primary intraventricular gliosarcoma. Clin Neuropathol. 2013;32:525–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous