

An Anatomic, Imaging, and Clinical Review of the Medial Longitudinal Fasciculus
- PMID: 33408958
- PMCID: PMC7771398
- DOI: 10.25259/JCIS_49_2020
An Anatomic, Imaging, and Clinical Review of the Medial Longitudinal Fasciculus
Abstract
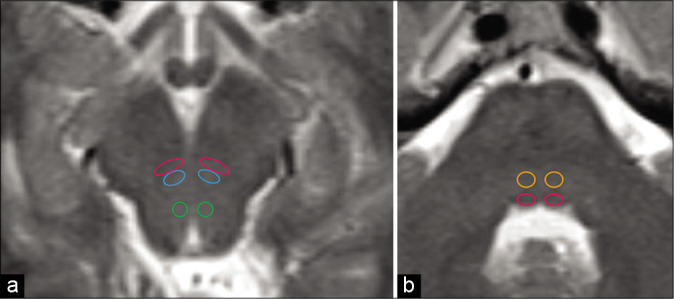
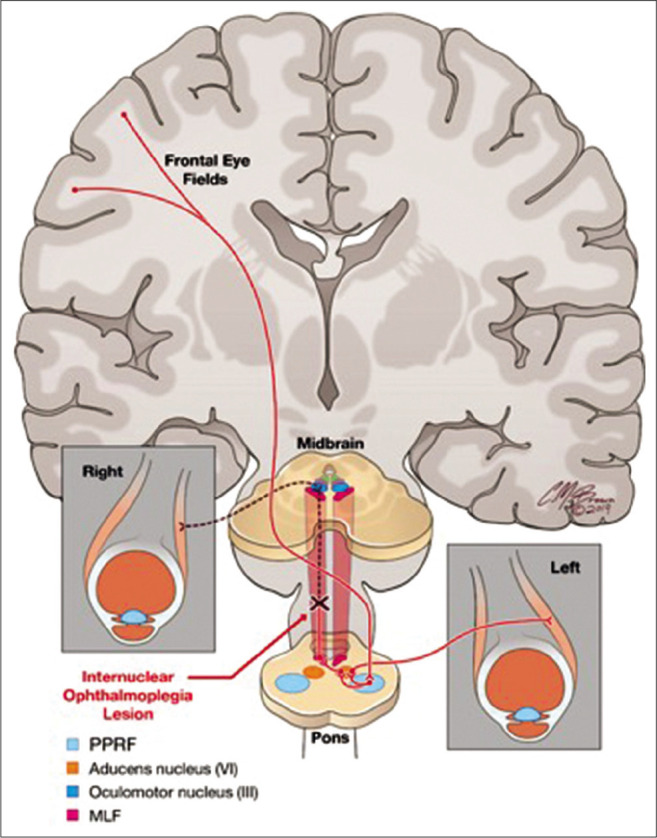
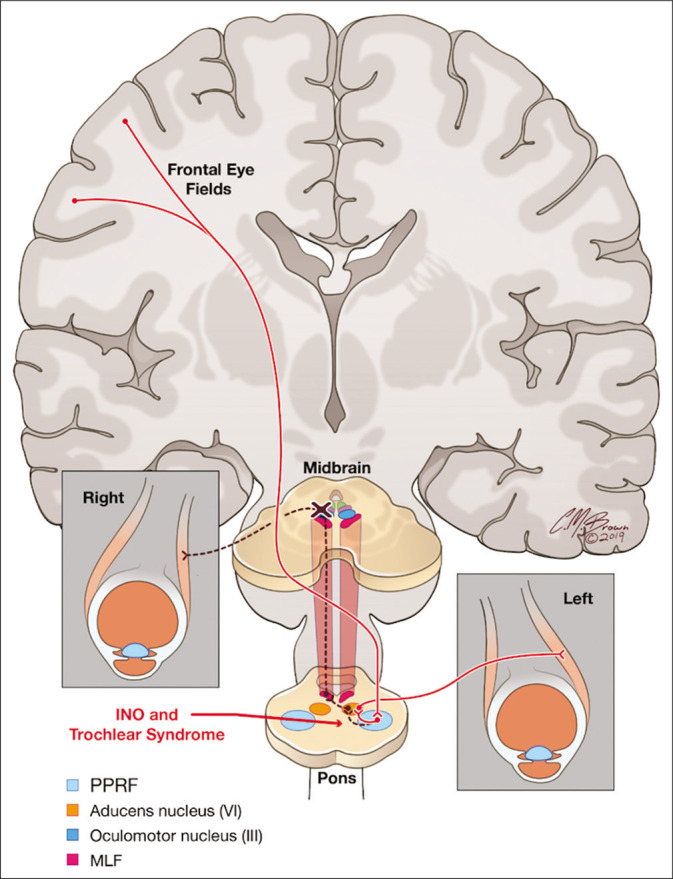
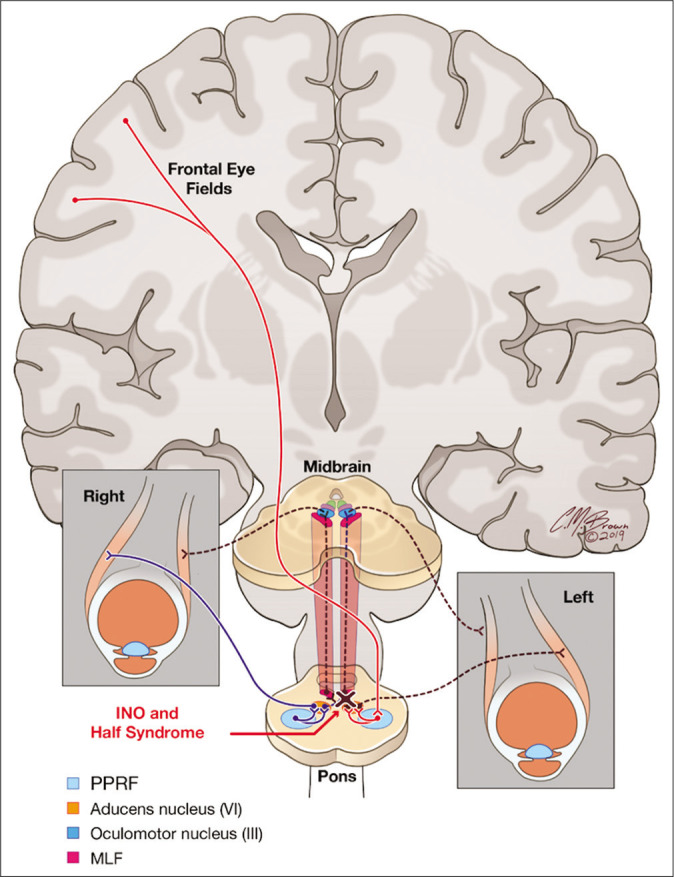
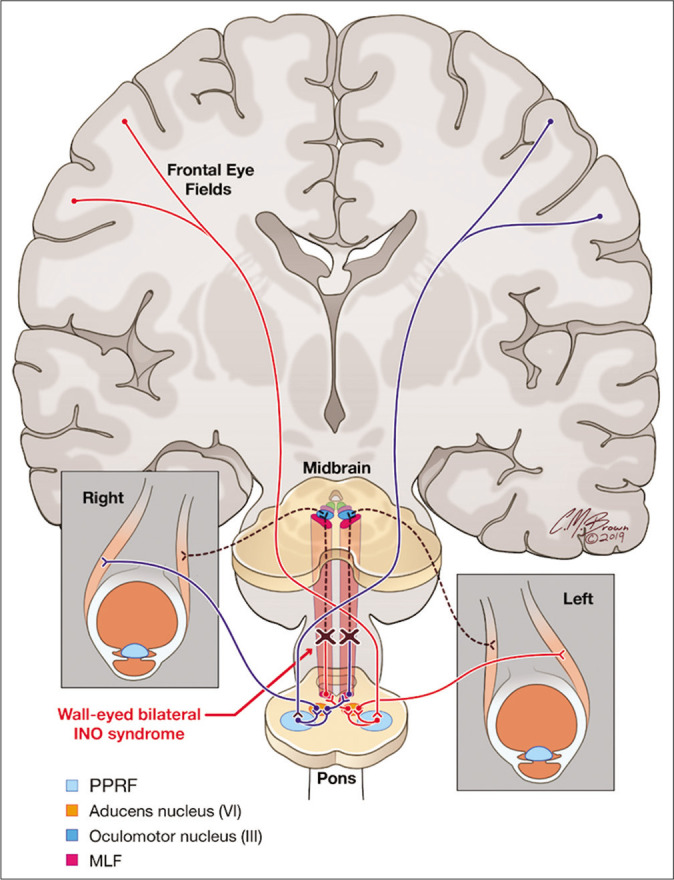
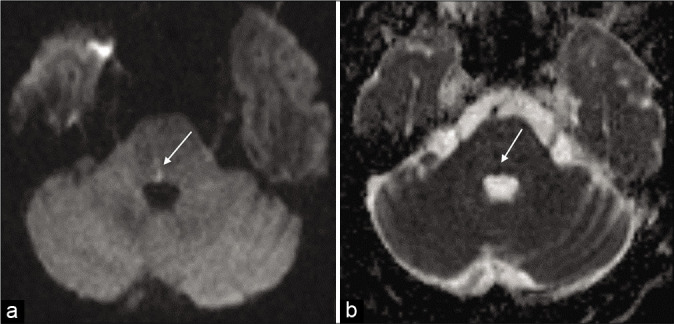
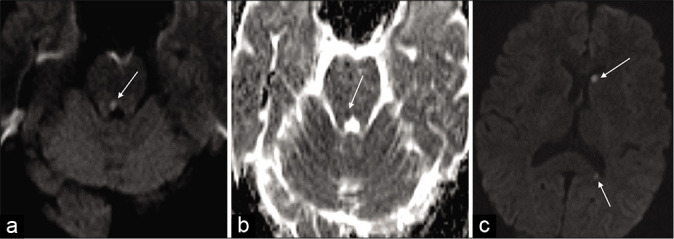
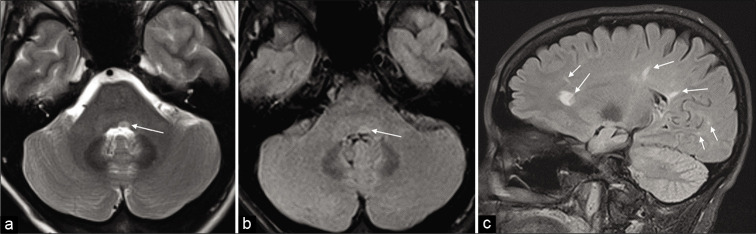
The medial longitudinal fasciculus (MLF) is a paired, highly specialized, and heavily myelinated nerve bundle responsible for extraocular muscle movements, including the oculomotor reflex, saccadic eye movements an smooth pursuit, and the vestibular ocular reflex. Clinically, lesions of the MLF are classically associated with internuclear ophthalmoplegia. However, clinical manifestations of a lesion in the MLF may be more complex and variable. We provide an overview of the neuroanatomy, neurologic manifestations, and correlative examples of the imaging findings on brain MRI of MLF lesions to provide the clinician and radiologist with a more comprehensive understanding of the MLF and potential clinical manifestations for an MLF lesion.
Keywords: Internuclear opthalmoplegia; Medial longitudinal fasciculus; One-and-a-half syndrome; Trochlear syndrome; Wall-eyed bilateral internuclear opthalmoparesis syndrome.
© 2020 Published by Scientific Scholar on behalf of Journal of Clinical Imaging Science.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources