

Influence of Hepatitis C Coinfection and Treatment on Risk of Diabetes Mellitus in HIV-Positive Persons
- PMID: 33409325
- PMCID: PMC7772946
- DOI: 10.1093/ofid/ofaa470
Influence of Hepatitis C Coinfection and Treatment on Risk of Diabetes Mellitus in HIV-Positive Persons
Abstract
Background: The role of hepatitis C virus (HCV) coinfection and HCV-RNA in the development of diabetes mellitus (DM) in HIV-positive persons remains unclear.
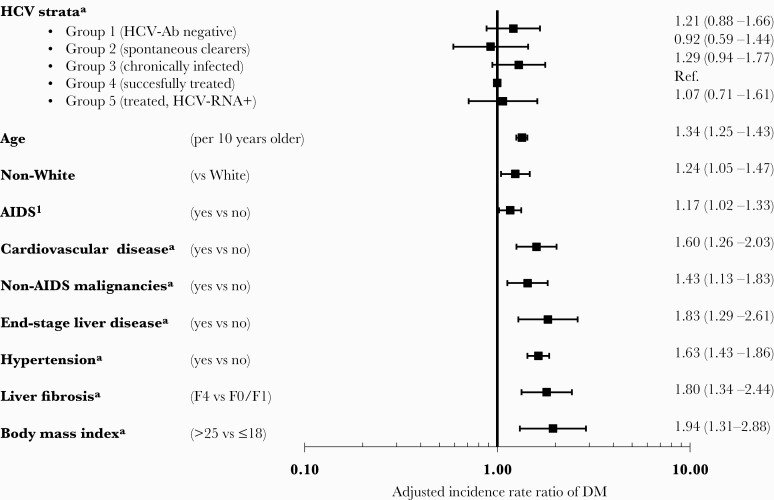
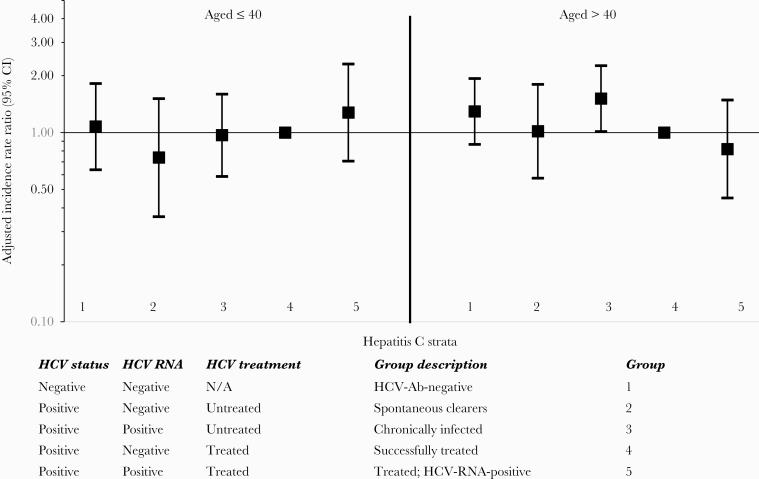
Methods: Poisson regression was used to compare incidence rates of DM (blood glucose >11.1 mmol/L, HbA1C >6.5% or >48 mmol/mol, starting antidiabetic medicine or physician reported date of DM onset) between current HIV/HCV groups (anti-HCV-negative, spontaneously cleared HCV, chronic untreated HCV, successfully treated HCV, HCV-RNA-positive after HCV treatment).
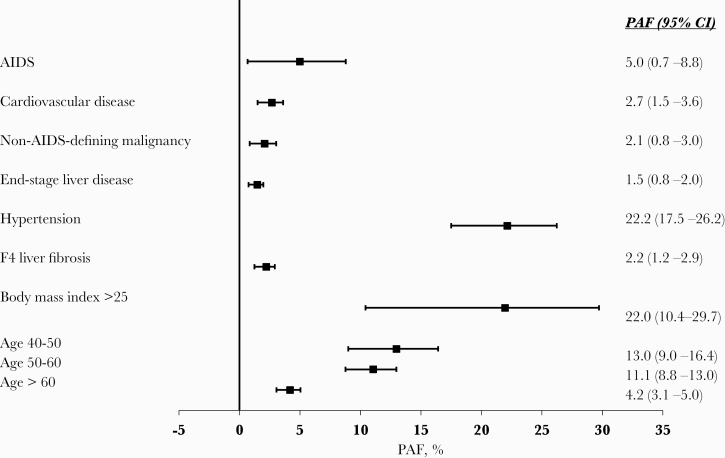
Results: A total of 16 099 persons were included; at baseline 10 091 (62.7%) were HCV-Ab-negative, 722 (4.5%) were spontaneous clearers, 3614 (22.4%) were chronically infected, 912 (5.7%) had been successfully treated, and 760 (4.7%) were HCV-RNA-positive after treatment. During 136 084 person-years of follow-up (PYFU; median [interquartile range], 6.9 [3.6-13.2]), 1108 (6.9%) developed DM (crude incidence rate, 8.1/1000 PYFU; 95% CI, 7.7-8.6). After adjustment, there was no difference between the 5 HCV strata in incidence of DM (global P = .33). Hypertension (22.2%; 95% CI, 17.5%-26.2%) and body mass index >25 (22.0%; 95% CI, 10.4%-29.7%) had the largest population-attributable fractions for DM.
Conclusions: HCV coinfection and HCV cure were not associated with DM in this large study. The biggest modifiable risk factors were hypertension and obesity, and continued efforts to manage such comorbidities should be prioritized.
Keywords: HIV; diabetes mellitus; direct-acting antivirals; hepatitis C; sustained virologic response.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Cacoub P, Gragnani L, Comarmond C, Zignego AL. Extrahepatic manifestations of chronic hepatitis C virus infection. Dig Liver Dis 2014; 46(Suppl 5):S165–73. - PubMed
-
- Dalrymple LS, Koepsell T, Sampson J, et al. . Hepatitis C virus infection and the prevalence of renal insufficiency. Clin J Am Soc Nephrol 2007; 2:715–21. - PubMed
-
- Lee MH, Yang HI, Lu SN, et al. ; R.E.V.E.A.L.-HCV Study Group Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. J Infect Dis 2012; 206:469–77. - PubMed
