

Single-cell RNA sequencing reveals compromised immune microenvironment in precursor stages of multiple myeloma
- PMID: 33409501
- PMCID: PMC7785110
- DOI: 10.1038/s43018-020-0053-3
Single-cell RNA sequencing reveals compromised immune microenvironment in precursor stages of multiple myeloma
Abstract
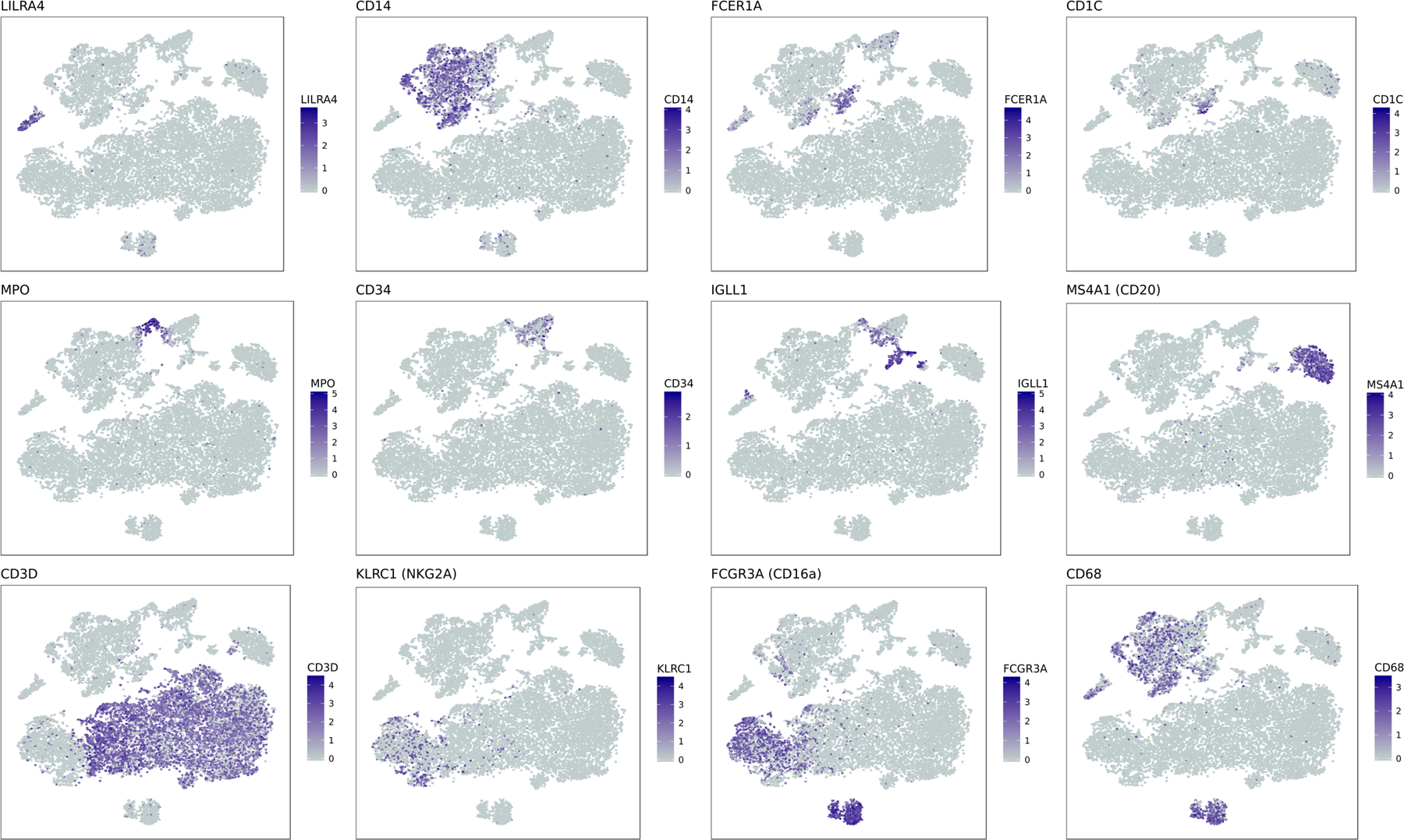
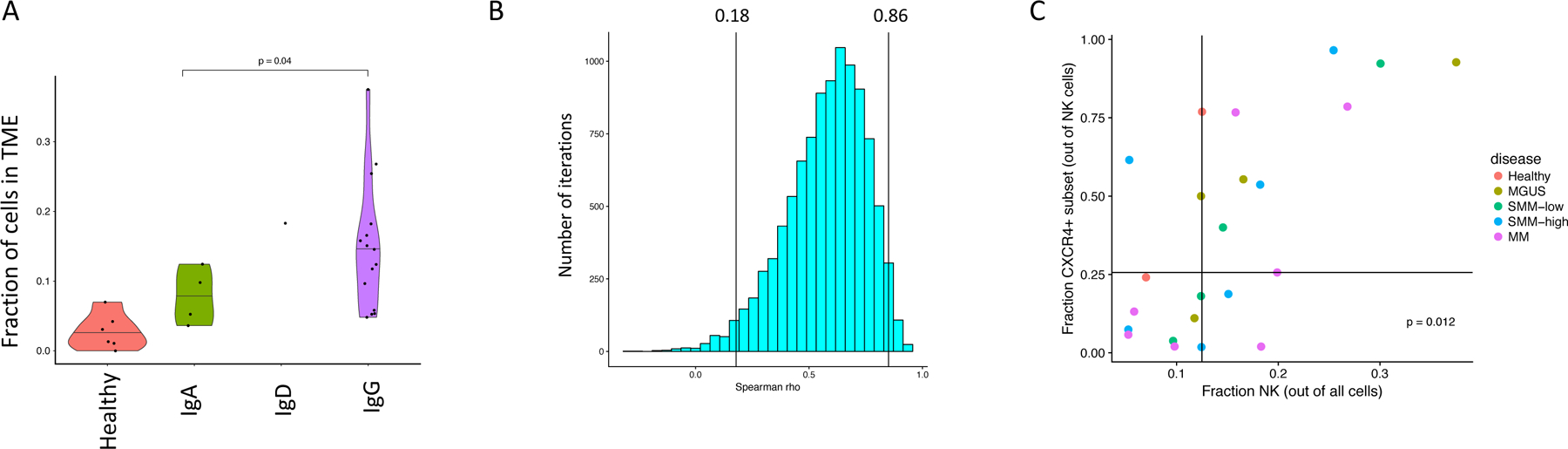
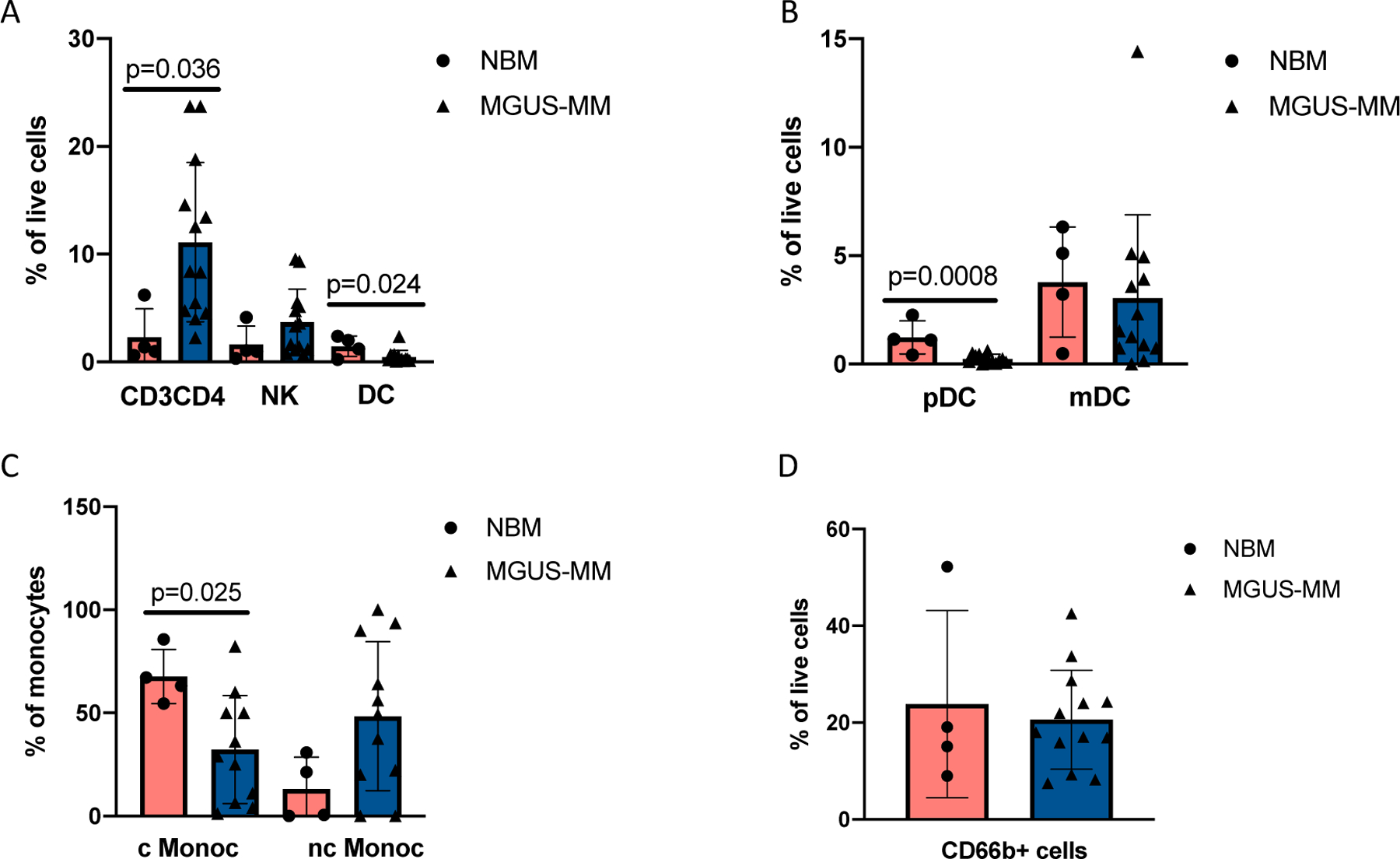
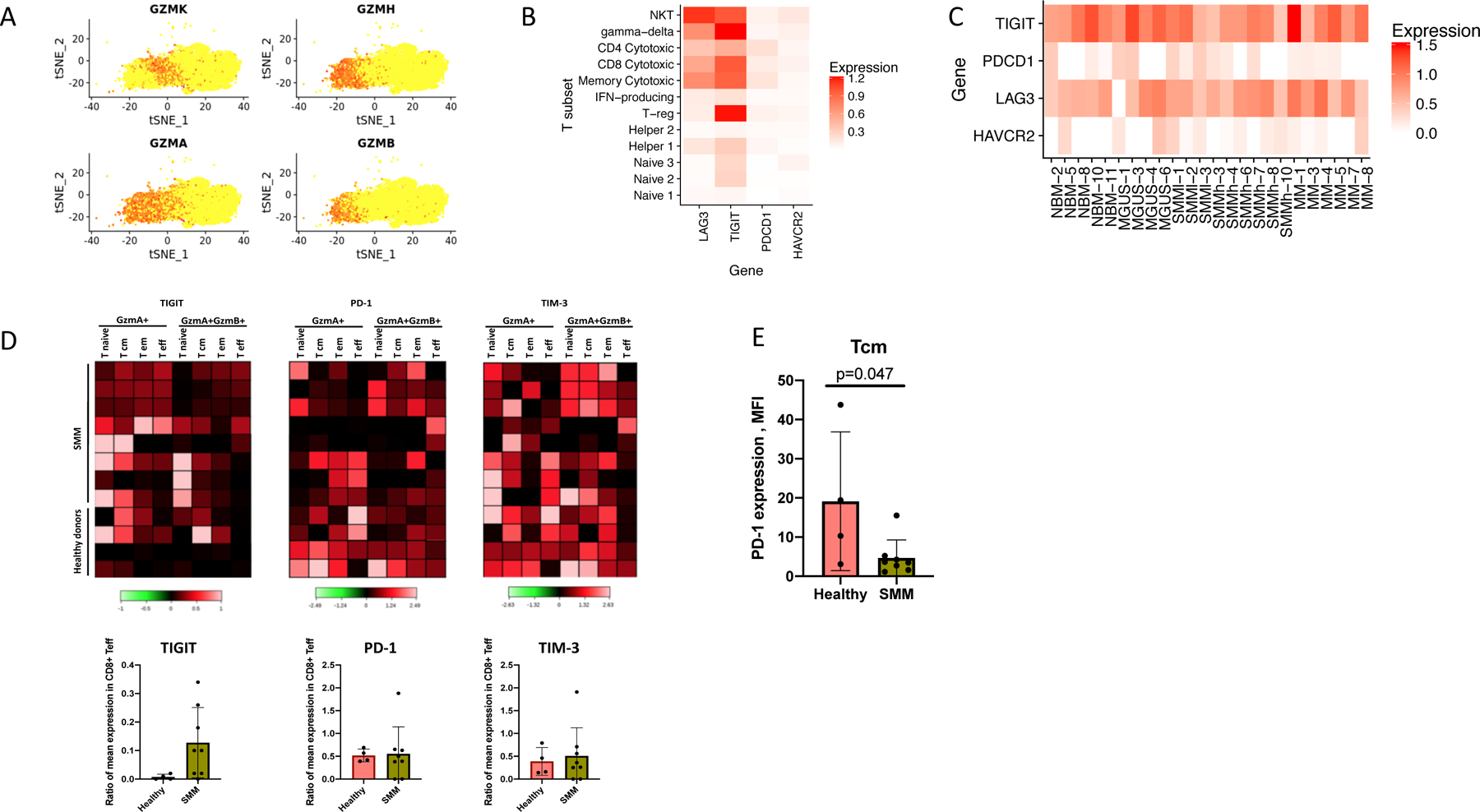
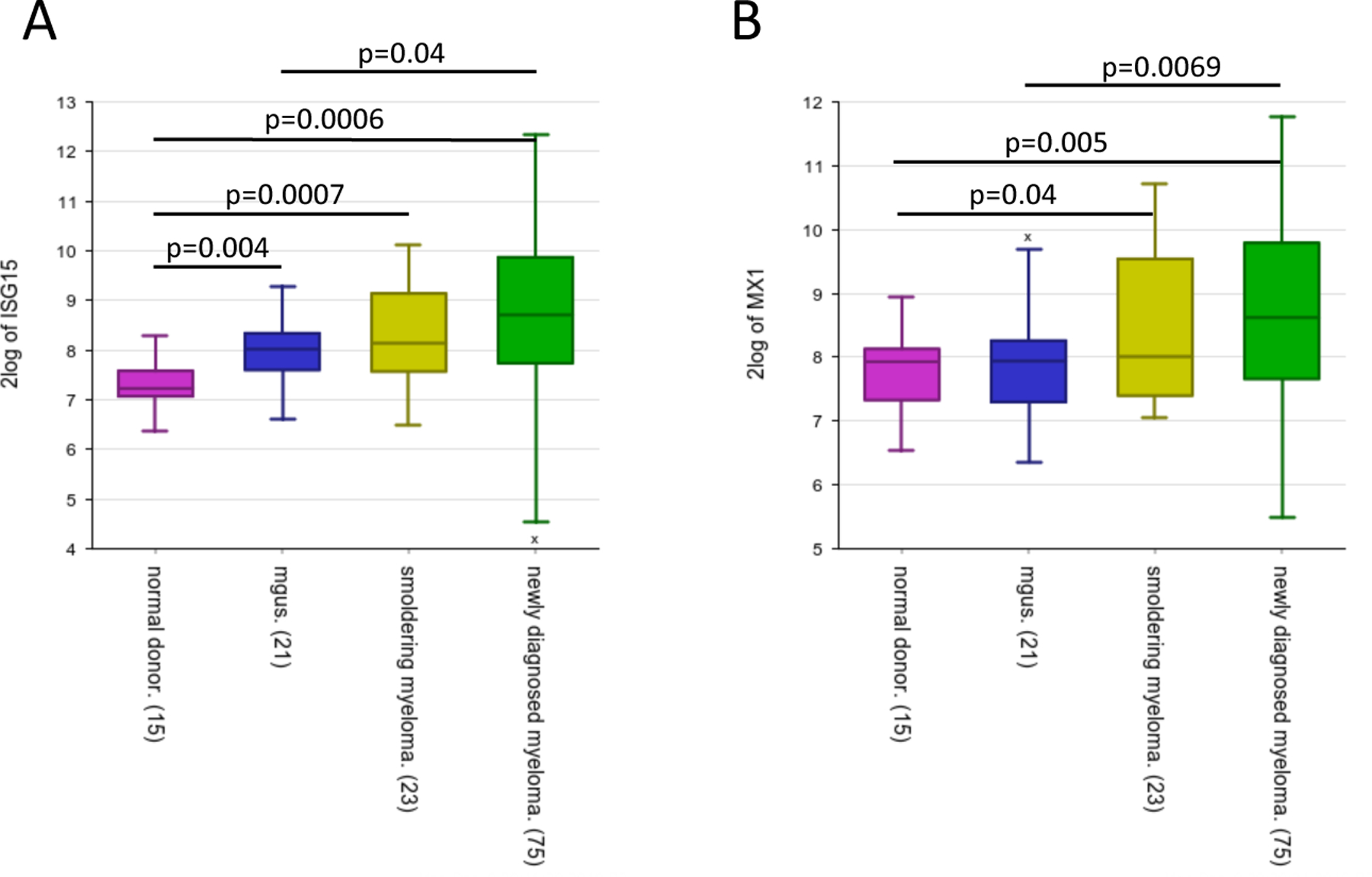
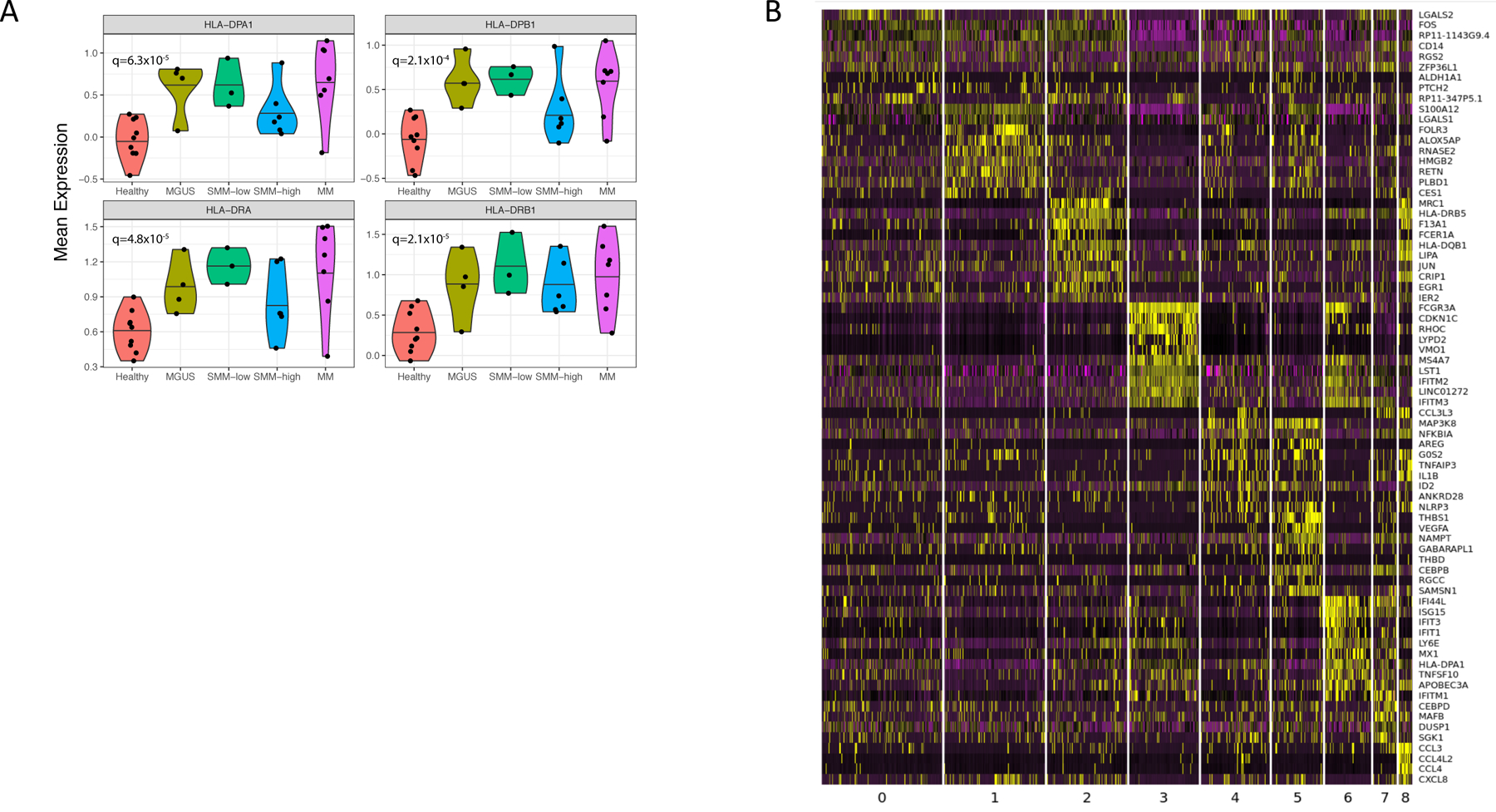
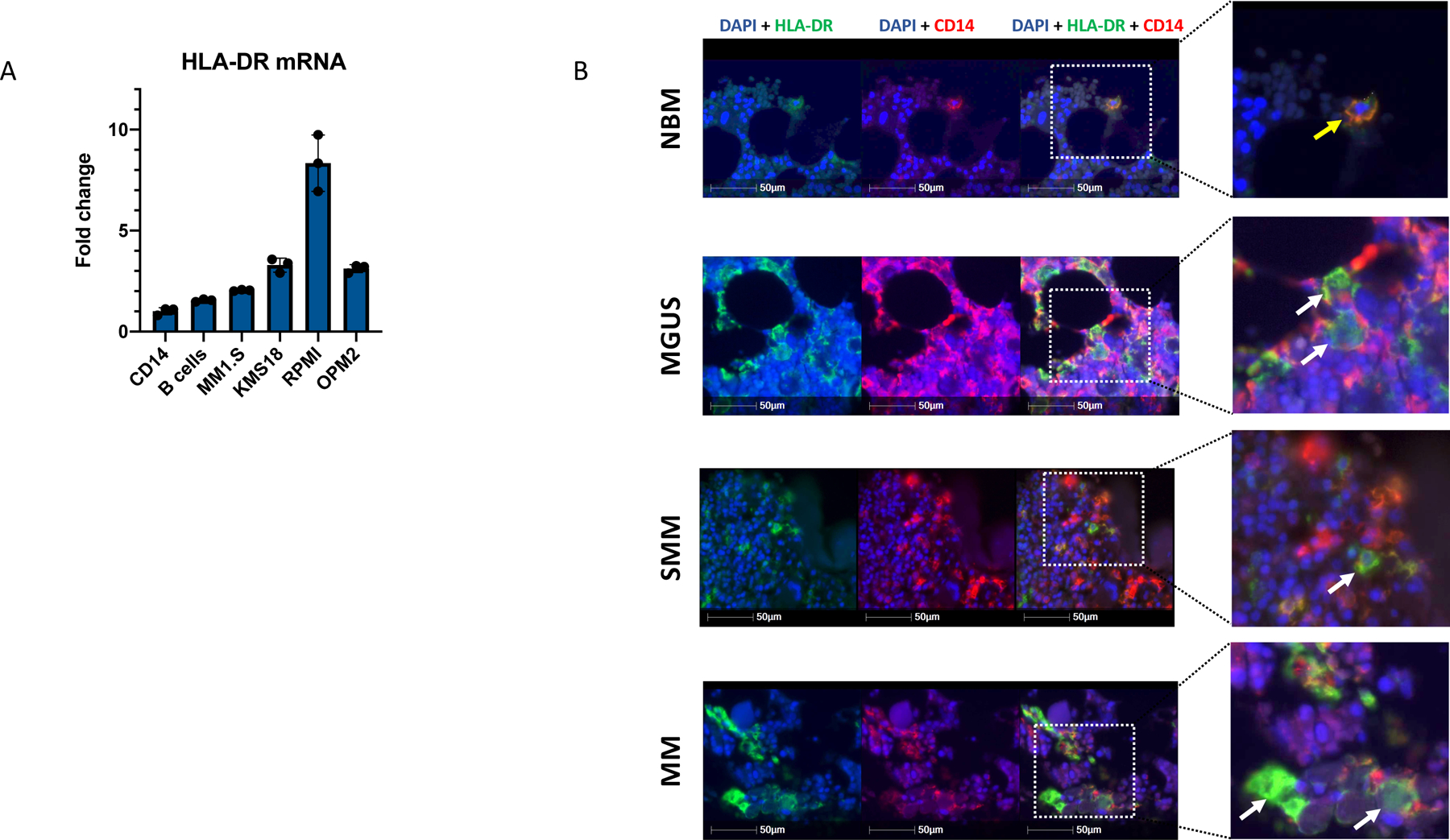
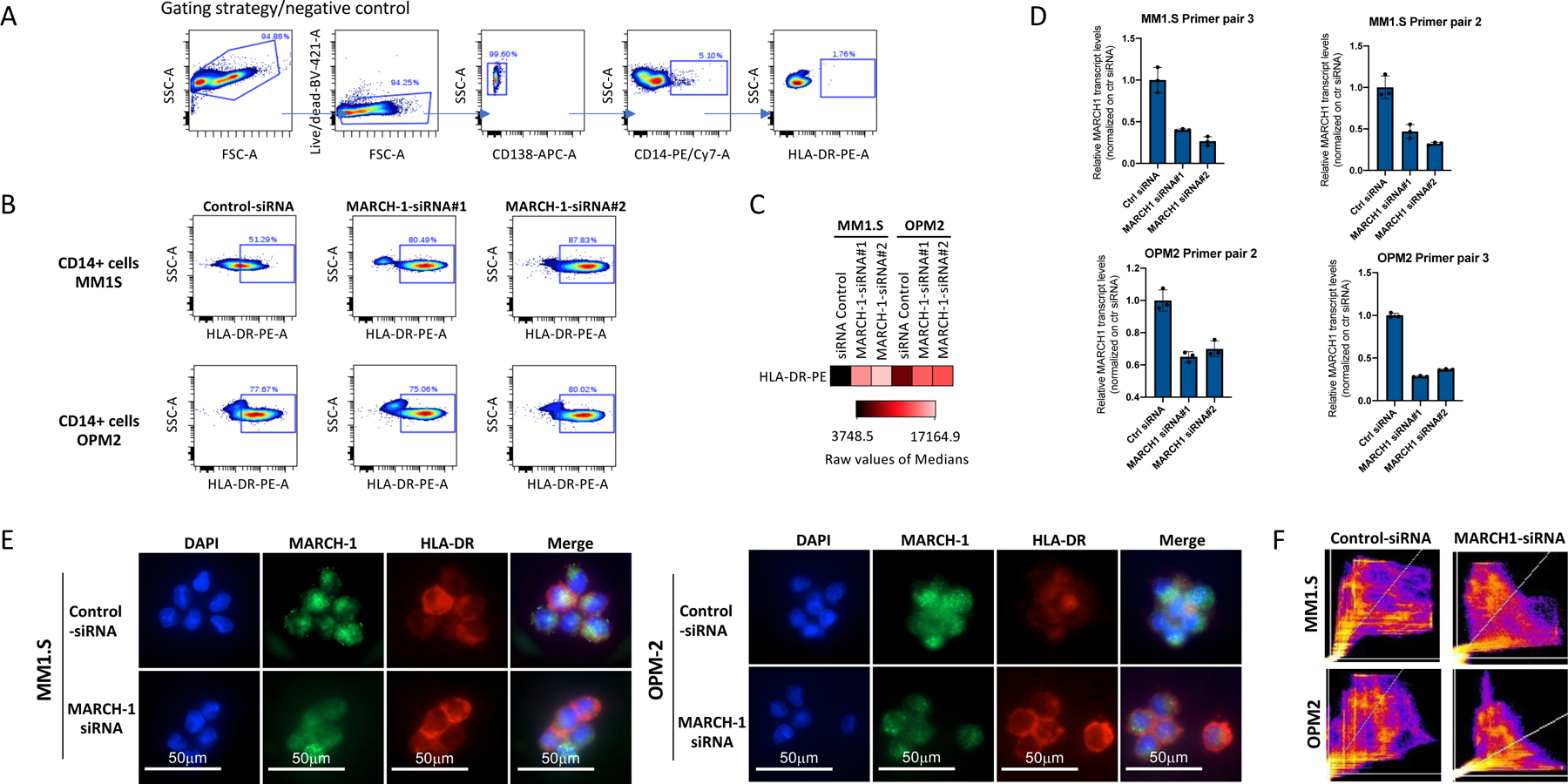
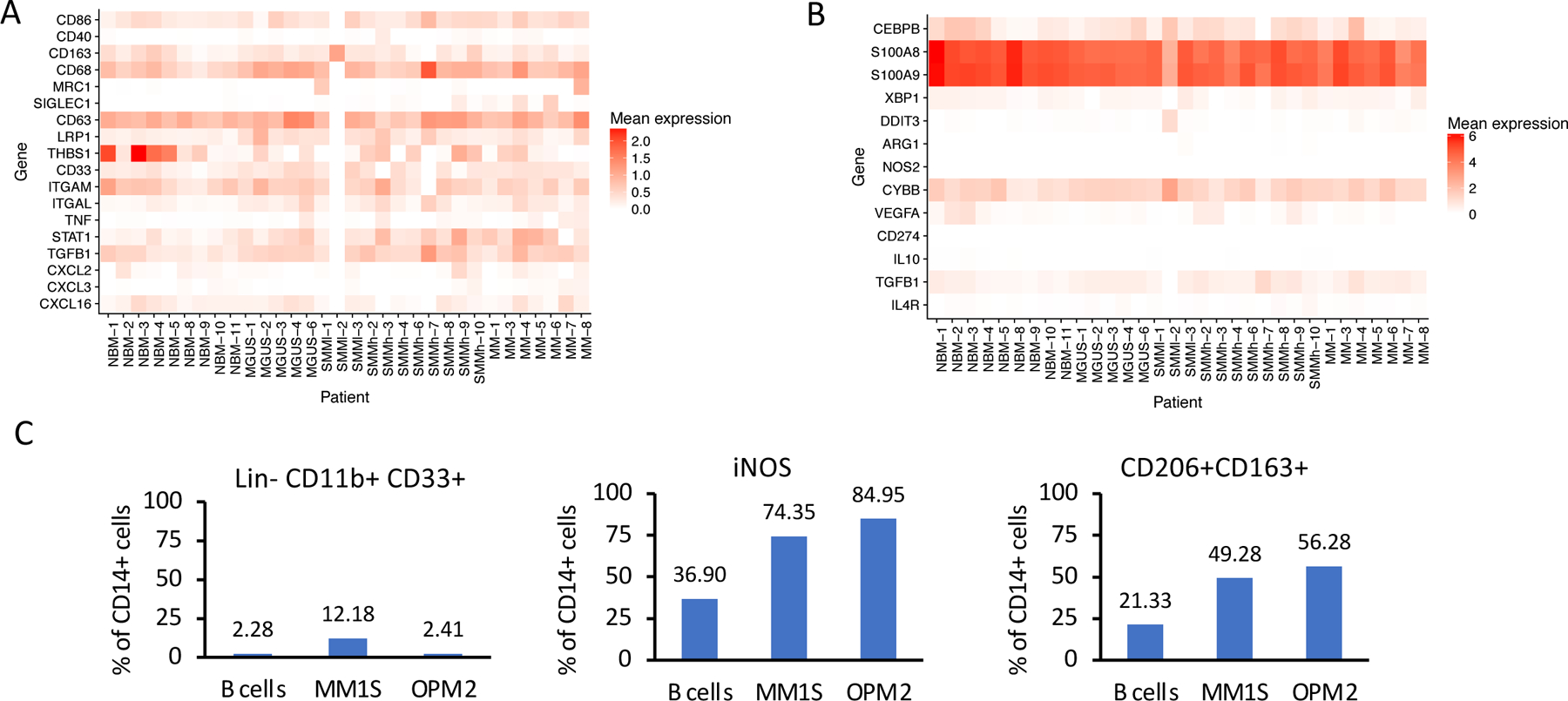
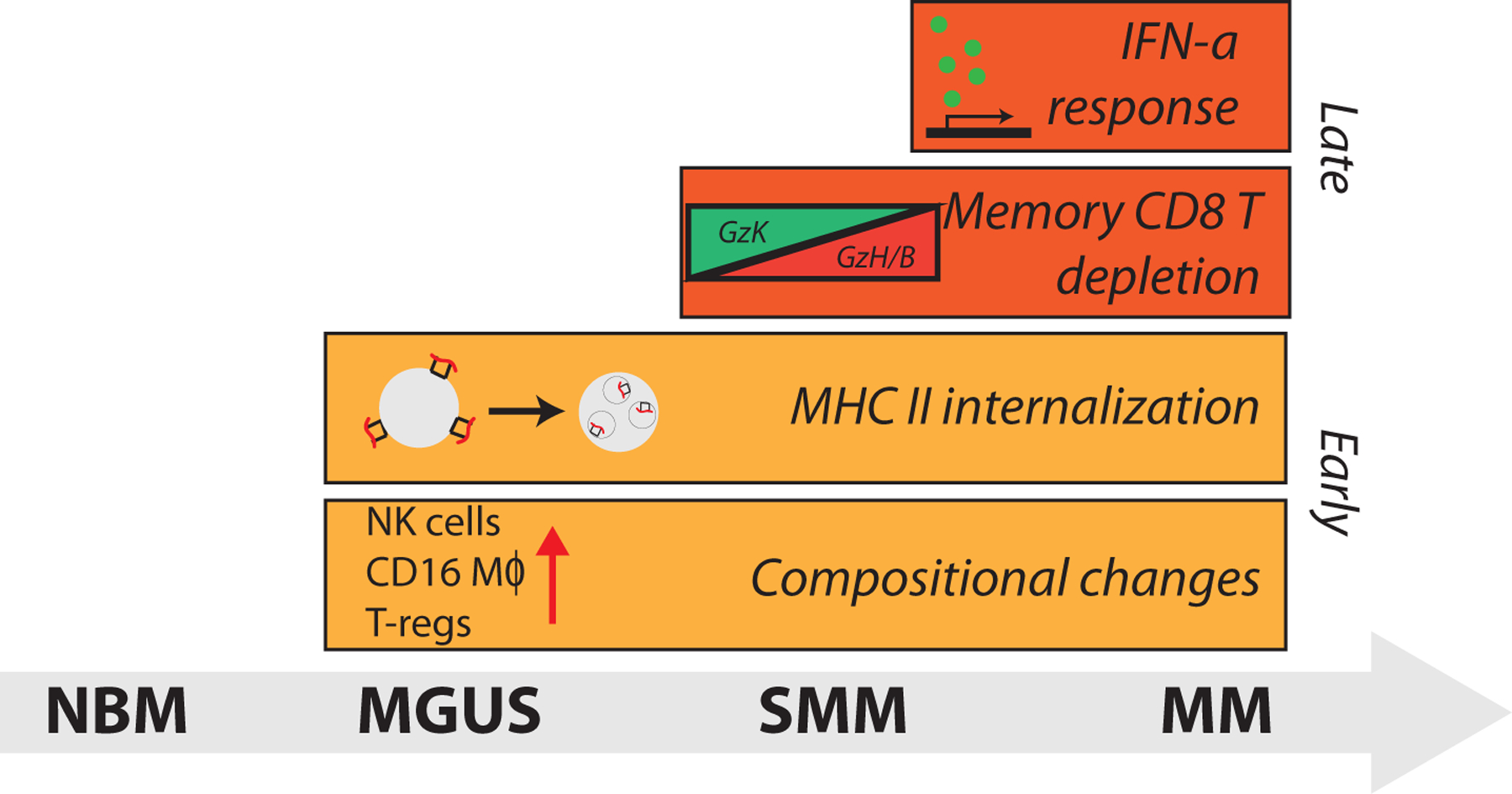
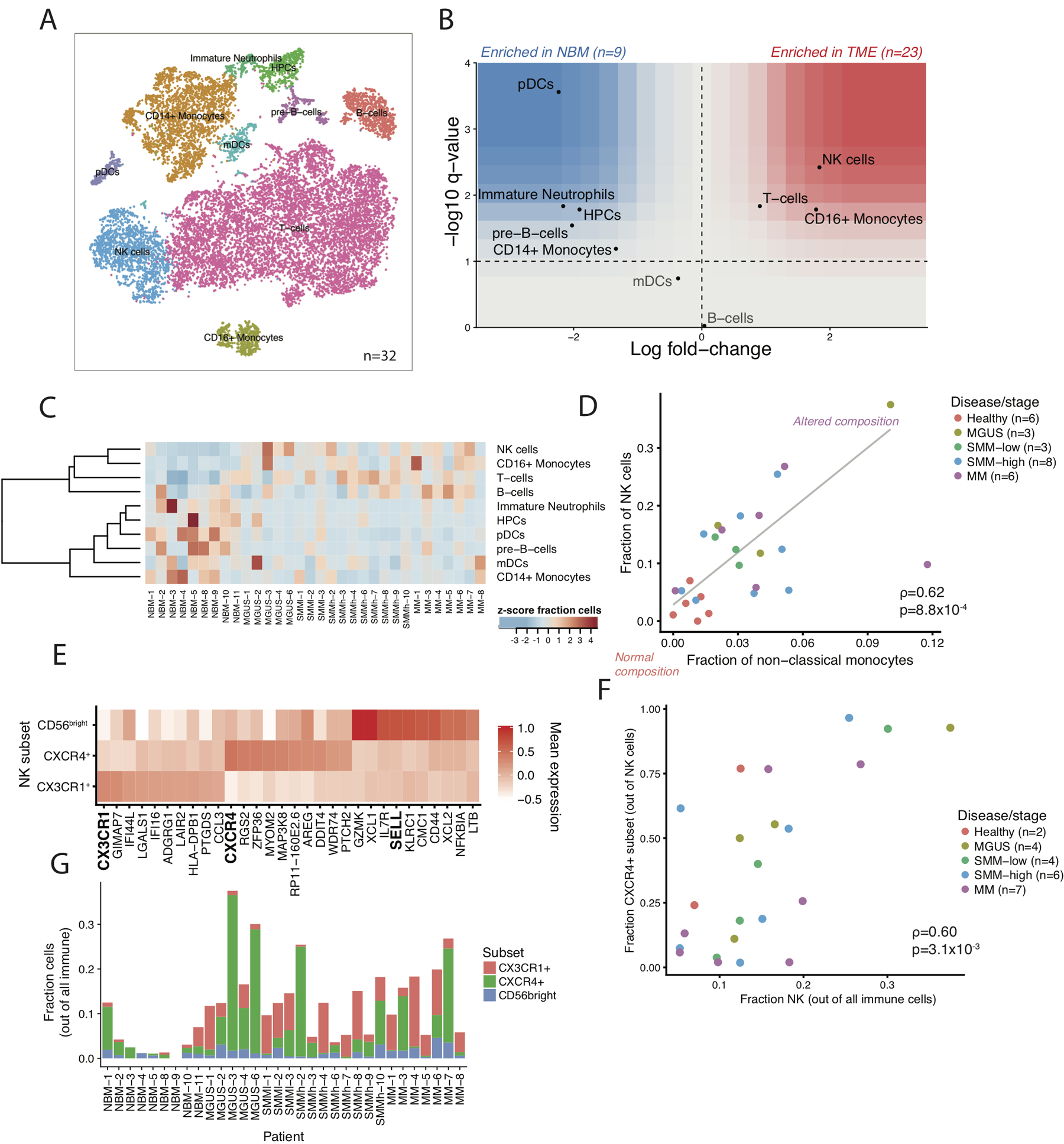
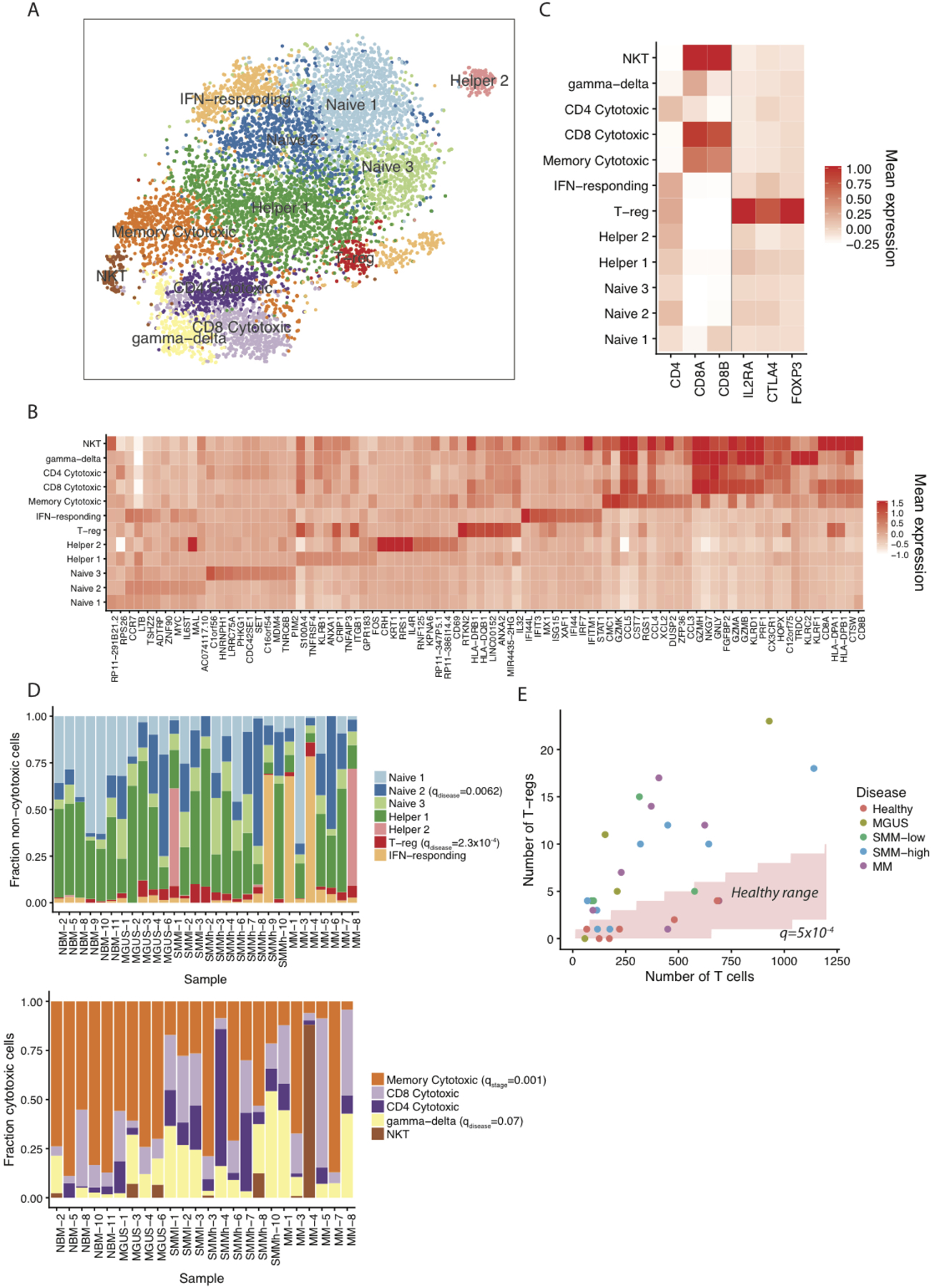
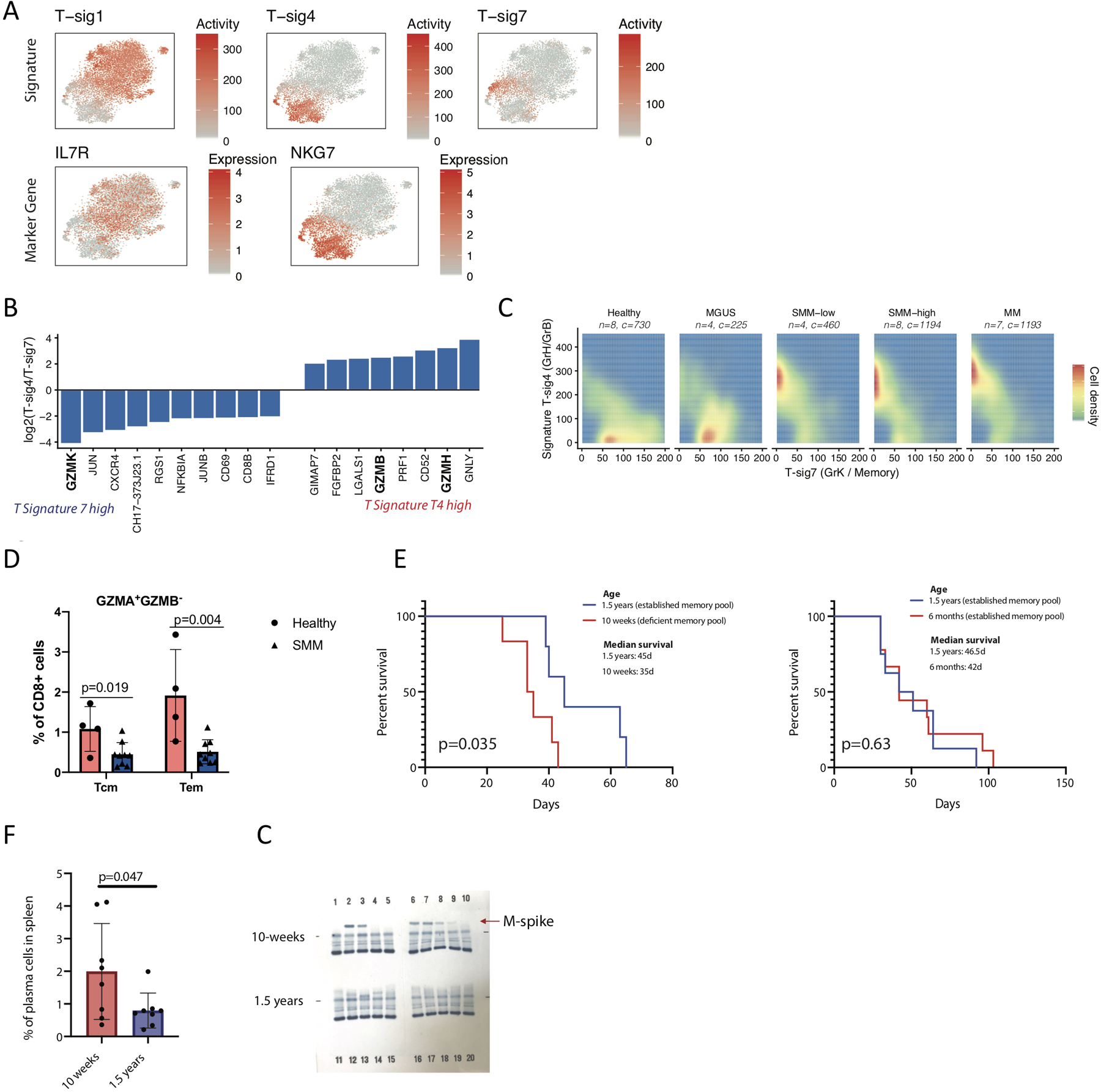
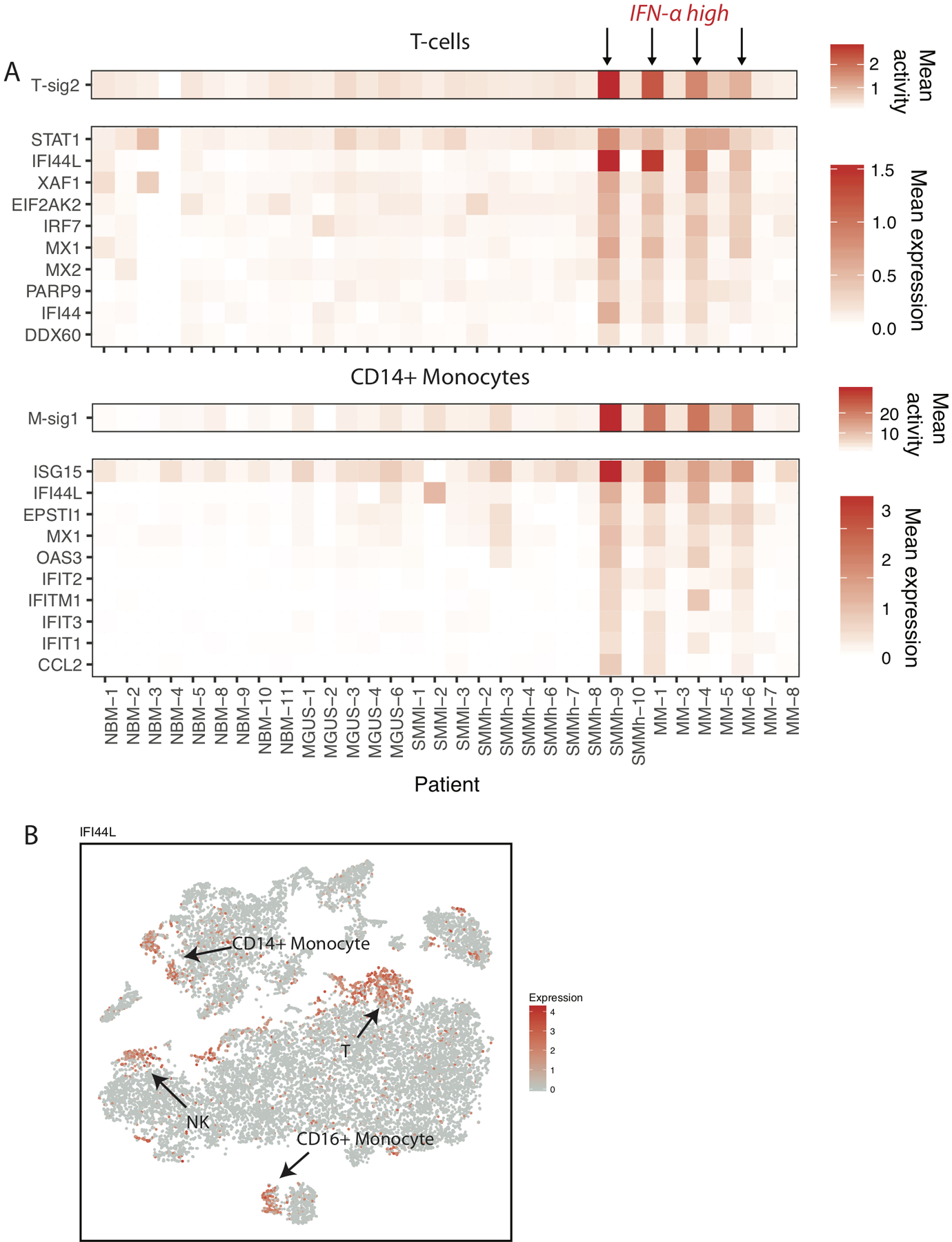
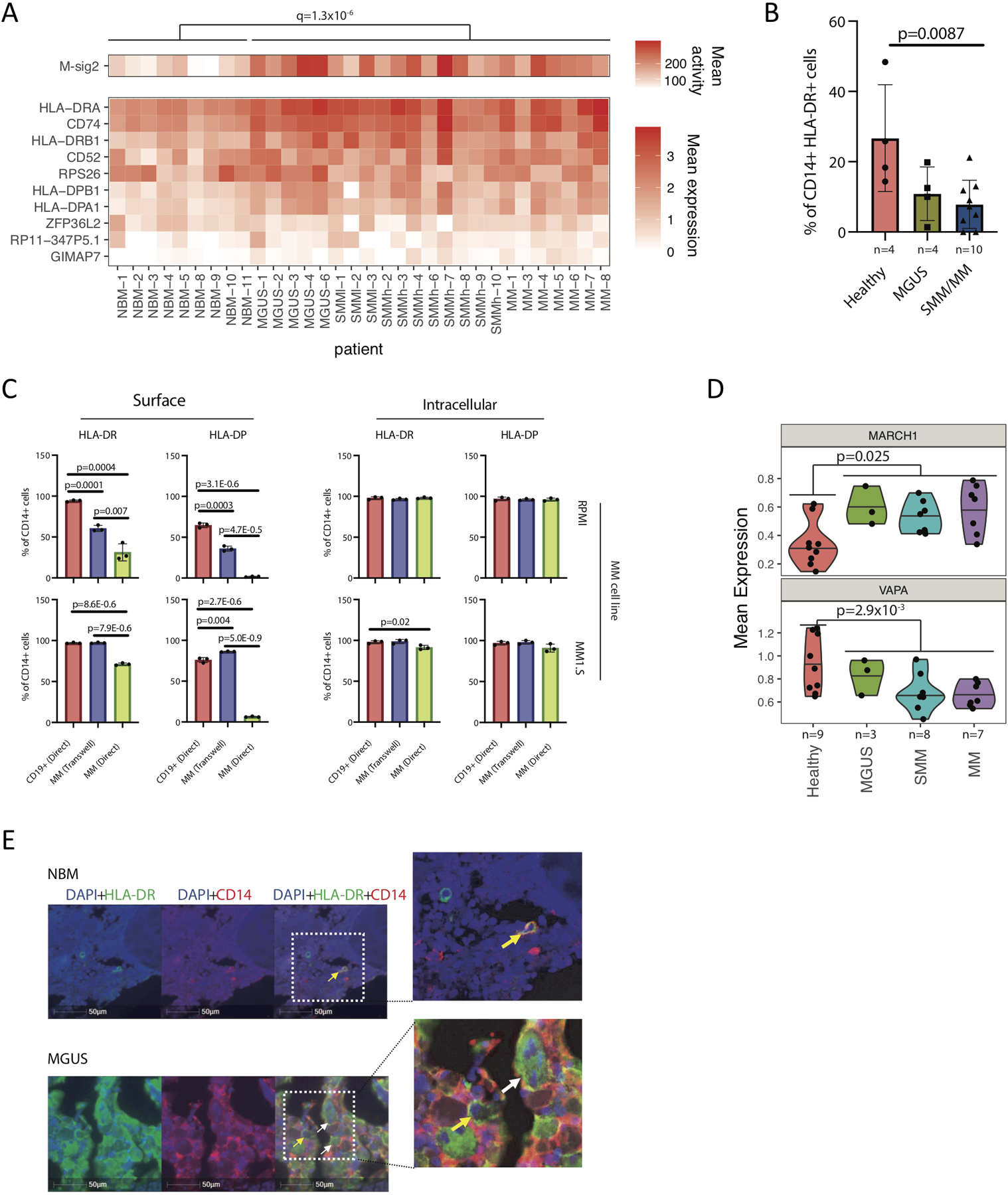
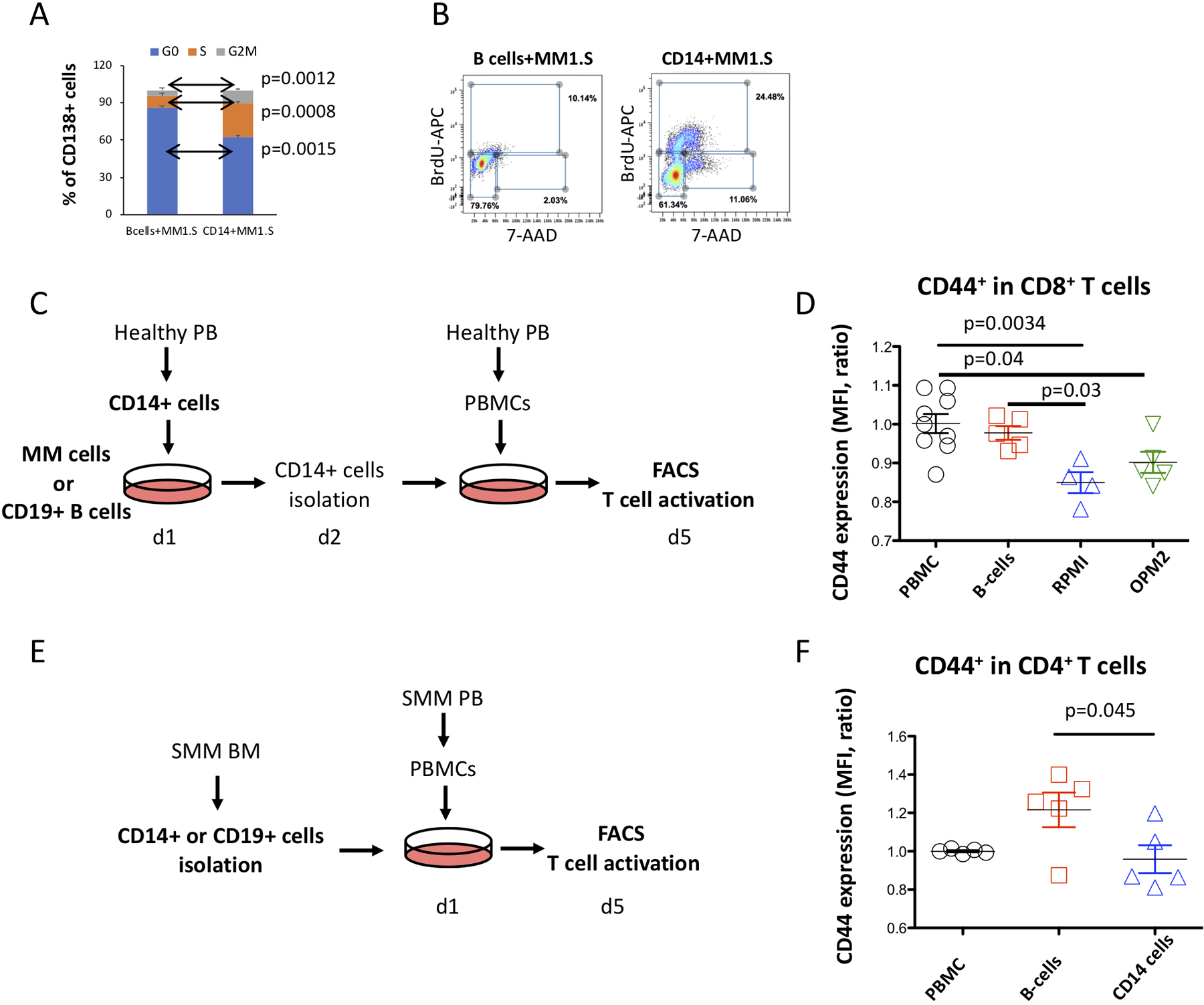
Precursor states of Multiple Myeloma (MM) and its native tumor microenvironment need in-depth molecular characterization to better stratify and treat patients at risk. Using single-cell RNA sequencing of bone marrow cells from precursor stages, MGUS and smoldering myeloma (SMM), to full-blown MM alongside healthy donors, we demonstrate early immune changes during patient progression. We find NK cell abundance is frequently increased in early stages, and associated with altered chemokine receptor expression. As early as SMM, we show loss of GrK+ memory cytotoxic T-cells, and show their critical role in MM immunosurveillance in mouse models. Finally, we report MHC class II dysregulation in CD14+ monocytes, which results in T cell suppression in vitro. These results provide a comprehensive map of immune changes at play over the evolution of pre-malignant MM, which will help develop strategies for immune-based patient stratification.
Keywords: MGUS; SMM; immune microenvironment; multiple myeloma; plasma cells; single-cell RNA sequencing; tumor microenvironment.
Conflict of interest statement
COMPETING INTERESTS STATEMENT G.G. receives research funds from IBM and Pharmacyclics. I.M.G. has a consulting/advisory role with GSK, AbbVie, Bristol-Myers Squibb (BMS). I.M.G has a consulting role with Sanofi, Janssen, Takeda, Celgene, Karyopharm, GNS, Cellectar, Medscape, Genetech, Adaptive, Aptitude, Curio Science, Magenta, Oncopeptides. I.M.G. received research funding/ honoraria from Celgene, Takeda, BMS, Janssen Pharmaceuticals, and Amgen.
Figures
Comment in
-
Stepwise immune alterations in multiple myeloma progression.Nat Cancer. 2020 May;1(5):477-479. doi: 10.1038/s43018-020-0063-1. Nat Cancer. 2020. PMID: 35121982 No abstract available.
References
-
- Kyle RA et al. Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management. Leukemia 24, 1121–1127, doi: 10.1038/leu.2010.60 (2010). - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
