

Adjuvant High-Flow Normobaric Oxygen After Mechanical Thrombectomy for Anterior Circulation Stroke: a Randomized Clinical Trial
- PMID: 33410112
- PMCID: PMC7787705
- DOI: 10.1007/s13311-020-00979-3
Adjuvant High-Flow Normobaric Oxygen After Mechanical Thrombectomy for Anterior Circulation Stroke: a Randomized Clinical Trial
Abstract
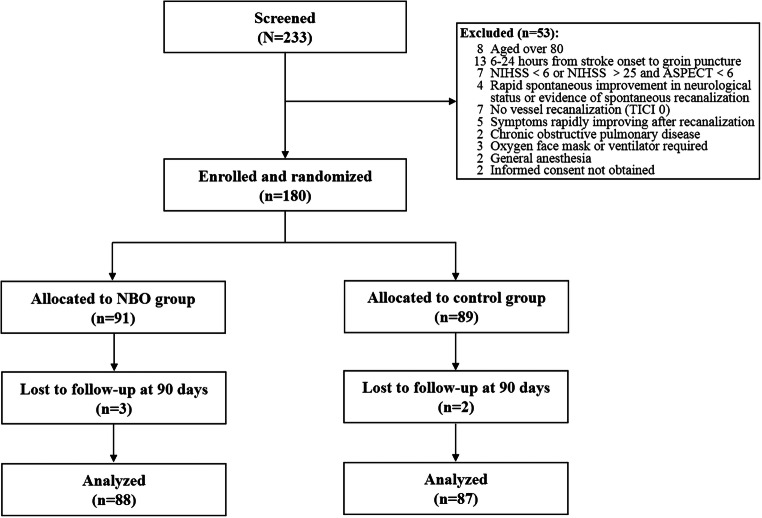
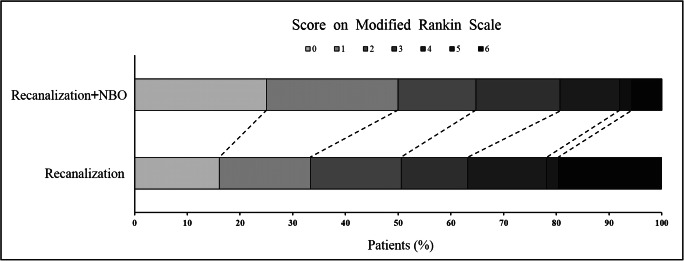
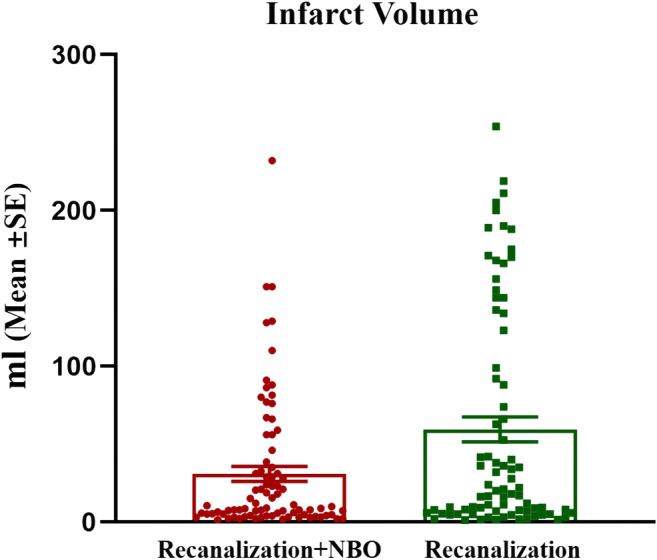
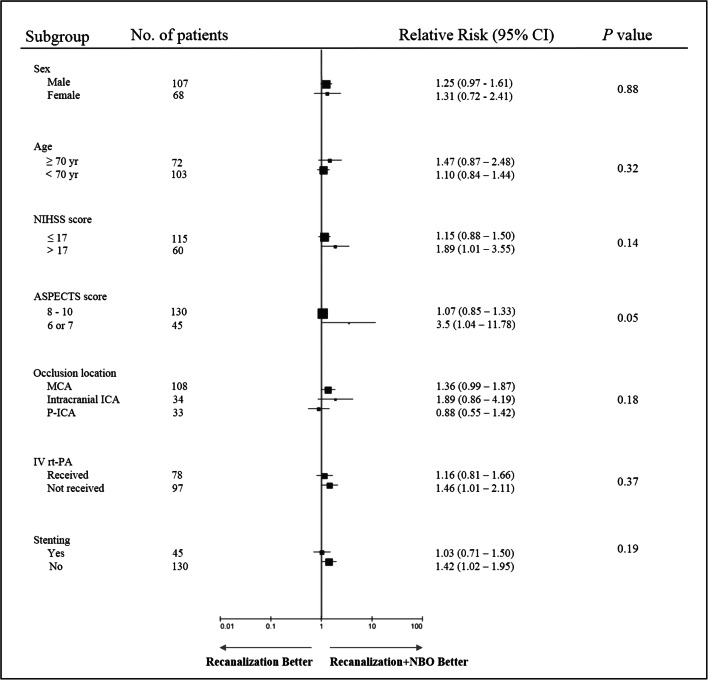
Adjuvant neuroprotective therapies for acute ischemic stroke (AIS) have demonstrated benefit in animal studies, albeit without human translation. We investigated the safety and efficacy of high-flow normobaric oxygen (NBO) after endovascular recanalization in anterior circulation stroke. This is a prospective randomized controlled study. Eligible patients were randomized to receive high-flow NBO by a Venturi mask (FiO2 50%, flow 15 L/min) or routine low-flow oxygen supplementation by nasal cannula (flow 3 L/min) after vessel recanalization for 6 h. Patient demographics, procedural metrics, complications, functional outcomes, symptomatic intracranial hemorrhage (sICH), and infarct volume were assessed. A total of 91 patients were treated with high-flow NBO. NBO treatment revealed a common odds ratio of 2.2 (95% CI, 1.26 to 3.87) favoring the distribution of global disability scores on the mRS at 90 days. The mortality at 90 days was significantly lower in the NBO group than in the control group, with an absolute difference of 13.86% (rate ratio, 0.35; 95% CI, 0.13-0.93). A significant reduction of infarct volume as determined by MRI was noted in the NBO group. The median infarct volume was 9.4 ml versus 20.5 ml in the control group (beta coefficient, - 20.24; 95% CI, - 35.93 to - 4.55). No significant differences were seen in the rate of sICH, pneumonia, urinary infection, and seizures between the 2 groups. This study suggests that high-flow NBO therapy after endovascular recanalization is safe and effective in improving functional outcomes, decreasing mortality, and reducing infarct volumes in anterior circulation stroke patients within 6 h from stroke onset.
Keywords: Oxygen supplement; endovascular recanalization; functional prognosis.; large vessel occlusion; neuroprotection.
© 2021. The American Society for Experimental NeuroTherapeutics, Inc.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
