

Timing, Distribution, and Relationship Between Nonpsychotic and Subthreshold Psychotic Symptoms Prior to Emergence of a First Episode of Psychosis
- PMID: 33410487
- PMCID: PMC8759816
- DOI: 10.1093/schbul/sbaa183
Timing, Distribution, and Relationship Between Nonpsychotic and Subthreshold Psychotic Symptoms Prior to Emergence of a First Episode of Psychosis
Abstract
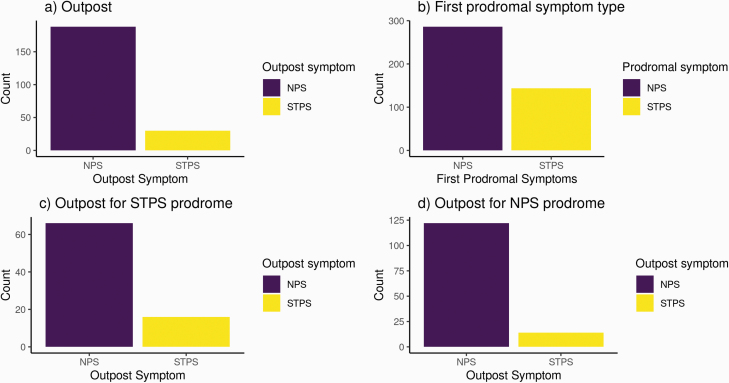
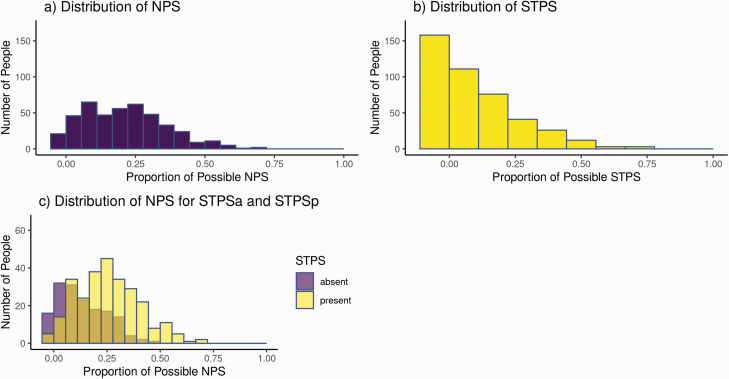
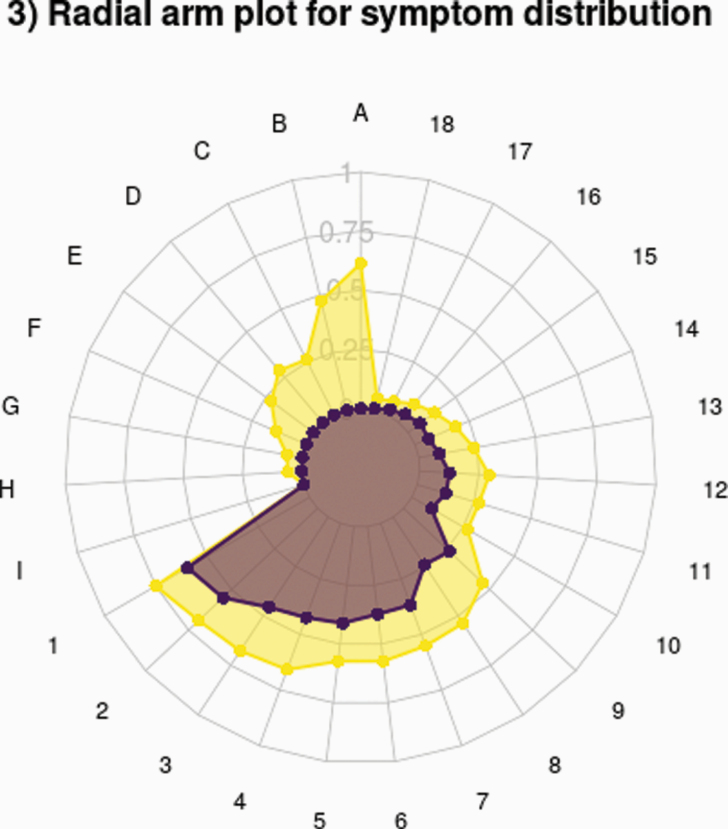
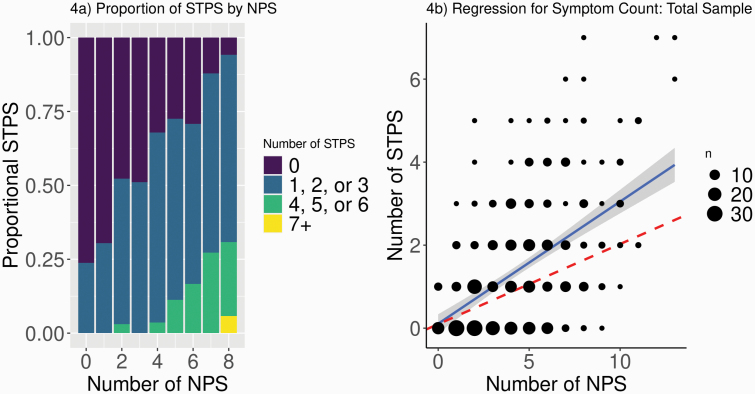
Prospective population studies suggest that psychotic syndromes may be an emergent phenomenon-a function of severity and complexity of more common mental health presentations and their nonpsychotic symptoms. Examining the relationship between nonpsychotic and subthreshold psychotic symptoms in individuals who later developed the ultimate outcome of interest, a first episode of psychosis (FEP), could provide valuable data to support or refute this conceptualization of how psychosis develops. We therefore conducted a detailed follow-back study consisting of semistructured interviews with 430 patients and families supplemented by chart reviews in a catchment-based sample of affective and nonaffective FEP. The onset and sequence of 27 pre-onset nonpsychotic (NPS) or subthreshold psychotic (STPS) symptoms was systematically characterized. Differences in proportions were analyzed with z-tests, and correlations were assessed with negative binomial regressions. Both the first psychiatric symptom (86.24% NPS) and the first prodromal symptom (66.51% NPS) were more likely to be NPS than STPS. Patients reporting pre-onset STPS had proportionally more of each NPS than did those without pre-onset STPS. Finally, there was a strong positive correlation between NPS counts (reflecting complexity) and STPS counts (β = 0.34, 95% CI [0.31, 0.38], P < 2 e-16). Prior to a FEP, NPS precede STPS, and greater complexity of NPS is associated with the presence and frequency of STPS. These findings complement recent arguments that the emergence of psychotic illness is better conceptualized as part of a continuum-with implications for understanding pluripotential developmental trajectories and strengthening early intervention paradigms.
Keywords: at-risk mental state; first-episode psychosis; psychopathology; psychosis; subthreshold psychotic symptoms; trajectory.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center.All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Resurrection of the Follow-Back Method to Study the Transdiagnostic Origins of Psychosis.Schizophr Bull. 2021 Apr 29;47(3):583-585. doi: 10.1093/schbul/sbab008. Schizophr Bull. 2021. PMID: 33543754 Free PMC article.
References
-
- van Os J. “ Schizophrenia” does not exist. Br Med J. 2016;352. http://search.proquest.com/openview/40c8d7375972dede6e1655927f8baa7e/1?p.... - PubMed
-
- Guloksuz S, van Os J. The slow death of the concept of schizophrenia and the painful birth of the psychosis spectrum. Psychol Med. 2018;48(2):229–244. - PubMed
-
- Zoghbi AW, Lieberman JA. Alive but not well: the limited validity but continued utility of the concept of schizophrenia. Psychol Med. 2018;48(2):245–246. - PubMed
-
- Lawrie SM, Hall J, McIntosh AM, Owens DG, Johnstone EC. The ‘continuum of psychosis’: scientifically unproven and clinically impractical. Br J Psychiatry. 2010;197(6):423–425. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
