

Implementation and Outcomes of Virtual Care Across a Tertiary Cancer Center During COVID-19
- PMID: 33410867
- PMCID: PMC7791400
- DOI: 10.1001/jamaoncol.2020.6982
Implementation and Outcomes of Virtual Care Across a Tertiary Cancer Center During COVID-19
Abstract
Importance: The coronavirus disease 2019 (COVID-19) pandemic has burdened health care resources and disrupted care of patients with cancer. Virtual care (VC) represents a potential solution. However, few quantitative data support its rapid implementation and positive associations with service capacity and quality.
Objective: To examine the outcomes of a cancer center-wide virtual care program in response to the COVID-19 pandemic.
Design, setting, and participants: This cohort study applied a hospitalwide agile service design to map gaps and develop a customized digital solution to enable at-scale VC across a publicly funded comprehensive cancer center. Data were collected from a high-volume cancer center in Ontario, Canada, from March 23 to May 22, 2020.
Main outcomes and measures: Outcome measures were care delivery volumes, quality of care, patient and practitioner experiences, and cost savings to patients.
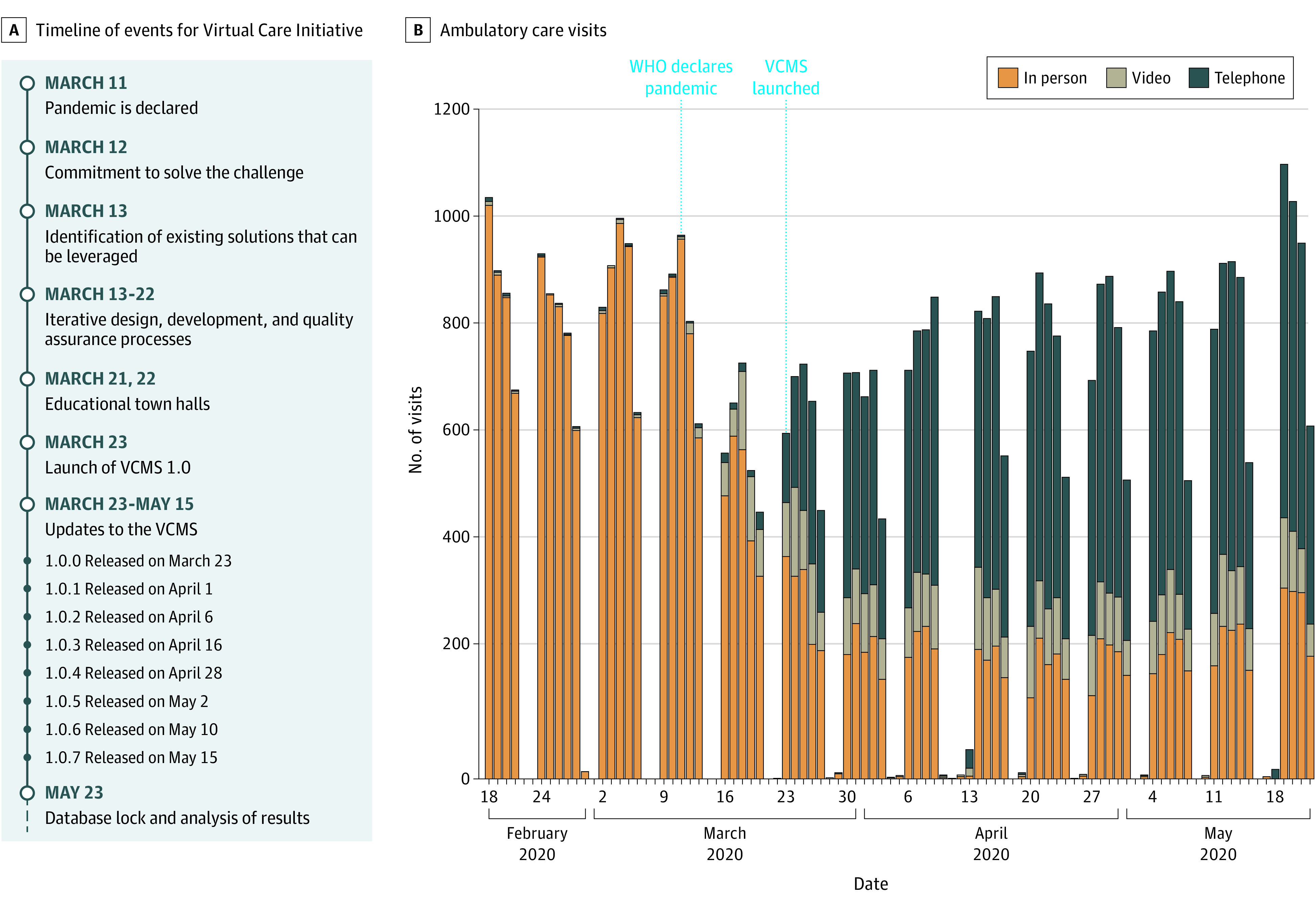
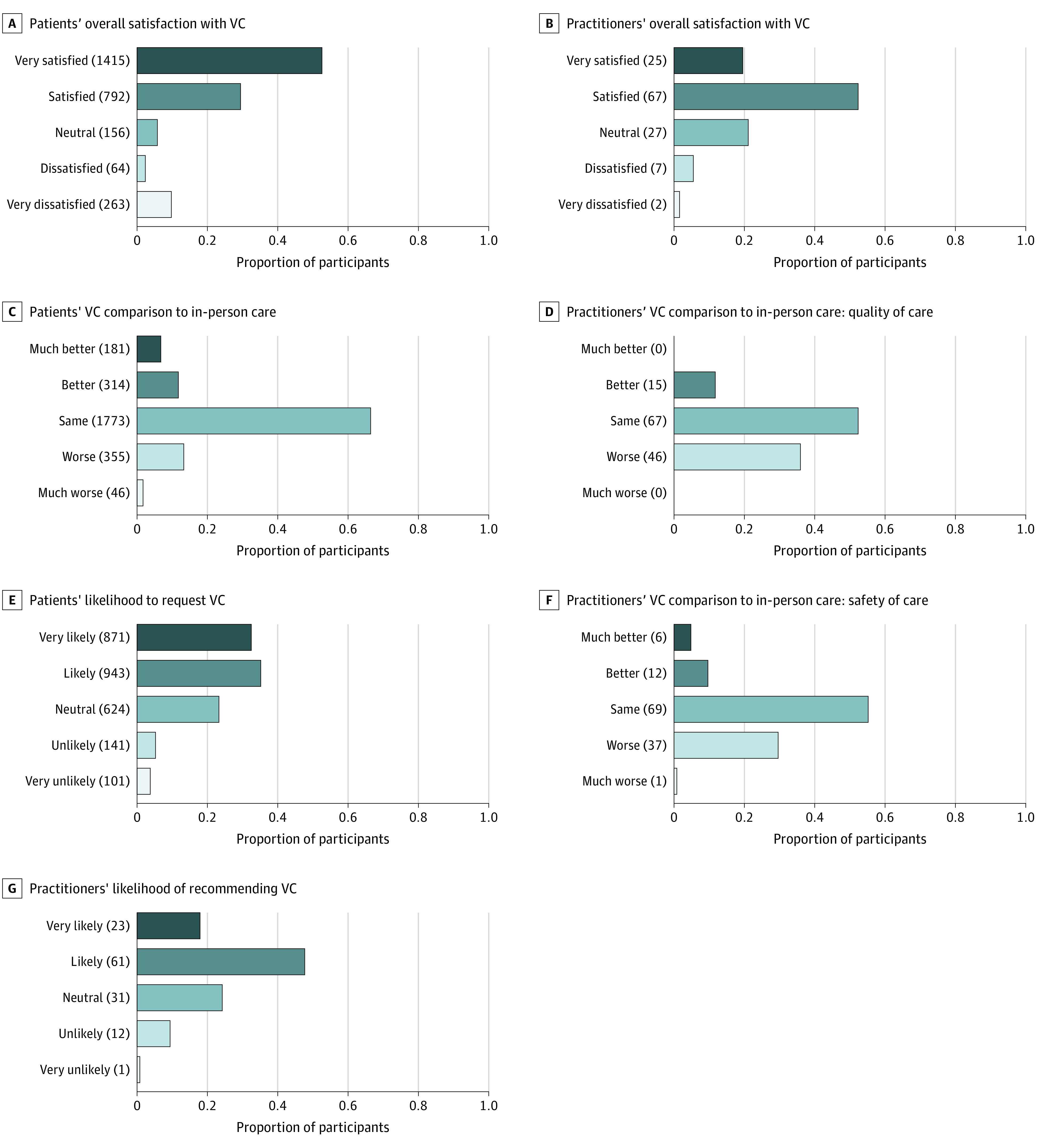
Results: The VC solution was developed and launched 12 days after the declaration of the COVID-19 pandemic. A total of 22 085 VC visits (mean, 514 visits per day) were conducted, comprising 68.4% (range, 18.8%-100%) of daily visits compared with 0.8% before launch (P < .001). Ambulatory clinic volumes recovered a month after deployment (3714-4091 patients per week), whereas chemotherapy and radiotherapy caseloads (1943-2461 patients per week) remained stable throughout. No changes in institutional or provincial quality-of-care indexes were observed. A total of 3791 surveys (3507 patients and 284 practitioners) were completed; 2207 patients (82%) and 92 practitioners (72%) indicated overall satisfaction with VC. The direct cost of this initiative was CAD$ 202 537, and displacement-related cost savings to patients totaled CAD$ 3 155 946.
Conclusions and relevance: These findings suggest that implementation of VC at scale at a high-volume cancer center may be feasible. An agile service design approach was able to preserve outpatient caseloads and maintain care quality, while rendering high patient and practitioner satisfaction. These findings may help guide the transformation of telemedicine in the post COVID-19 era.
Conflict of interest statement
Figures
Similar articles
-
Will virtual multidisciplinary team meetings become the norm for musculoskeletal oncology care following the COVID-19 pandemic? - experience from a tertiary sarcoma centre.BMC Musculoskelet Disord. 2021 Jan 5;22(1):18. doi: 10.1186/s12891-020-03925-8. BMC Musculoskelet Disord. 2021. PMID: 33402136 Free PMC article.
-
The reality of virtual care: Implications for cancer care beyond the pandemic.Healthc (Amst). 2020 Dec;8(4):100480. doi: 10.1016/j.hjdsi.2020.100480. Epub 2020 Oct 22. Healthc (Amst). 2020. PMID: 33129178 Free PMC article.
-
Positive impact of the pandemic: the effect of post-COVID-19 virtual visit implementation on departmental efficiency and patient satisfaction in a quaternary care center.Neurosurg Focus. 2022 Jun;52(6):E10. doi: 10.3171/2022.3.FOCUS2243. Neurosurg Focus. 2022. PMID: 35921181
-
Community oncology in an era of payment reform.Am Soc Clin Oncol Educ Book. 2014:e447-52. doi: 10.14694/EdBook_AM.2014.34.e447. Am Soc Clin Oncol Educ Book. 2014. PMID: 24857138 Review.
-
COVID-19 and telepsychiatry: Early outpatient experiences and implications for the future.Gen Hosp Psychiatry. 2020 Sep-Oct;66:89-95. doi: 10.1016/j.genhosppsych.2020.07.002. Epub 2020 Jul 9. Gen Hosp Psychiatry. 2020. PMID: 32750604 Free PMC article. Review.
Cited by
-
Telemedicine in Cancer Care Beyond the COVID-19 Pandemic: Oncology 2.0?Curr Oncol Rep. 2022 Dec;24(12):1843-1850. doi: 10.1007/s11912-022-01332-x. Epub 2022 Oct 8. Curr Oncol Rep. 2022. PMID: 36208400 Free PMC article. Review.
-
The Logistics of Medication and Patient Flow in Video-Based Virtual Clinics During a Sudden COVID-19 Outbreak in Taiwan: Observational Study.Interact J Med Res. 2022 Jun 10;11(1):e37880. doi: 10.2196/37880. Interact J Med Res. 2022. PMID: 35687404 Free PMC article.
-
Virtual Care and Electronic Patient Communication During COVID-19: Cross-sectional Study of Inequities Across a Canadian Tertiary Cancer Center.J Med Internet Res. 2022 Nov 4;24(11):e39728. doi: 10.2196/39728. J Med Internet Res. 2022. PMID: 36331536 Free PMC article.
-
Survey of the Impact of COVID-19 on Chronic Liver Disease Patient Care Experiences and Outcomes.J Can Assoc Gastroenterol. 2022 Jul 18;6(1):8-16. doi: 10.1093/jcag/gwac022. eCollection 2023 Feb. J Can Assoc Gastroenterol. 2022. PMID: 36785575 Free PMC article.
-
Delivery of Virtual Care in Oncology: Province-Wide Interprofessional Consensus Statements Using a Modified Delphi Process.Curr Oncol. 2021 Dec 13;28(6):5332-5345. doi: 10.3390/curroncol28060445. Curr Oncol. 2021. PMID: 34940084 Free PMC article.
References
-
- Pan American Health Organization . Framework for the Implementation of a Telemedicine Service. Pan American Health Organization; 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
