

Diagnostic Value of Patient-Reported and Clinically Tested Olfactory Dysfunction in a Population Screened for COVID-19
- PMID: 33410887
- PMCID: PMC7791399
- DOI: 10.1001/jamaoto.2020.5074
Diagnostic Value of Patient-Reported and Clinically Tested Olfactory Dysfunction in a Population Screened for COVID-19
Abstract
Importance: Recent studies have suggested that olfactory dysfunction and gustatory dysfunction are associated with coronavirus disease 2019 (COVID-19). However, olfaction has been evaluated solely on reported symptoms, after COVID-19 diagnosis, and in both mild and severe COVID-19 cases, but rarely has it been assessed in prospectively unselected populations.
Objective: To evaluate the diagnostic value of a semiobjective olfactory test developed to assess patient-reported chemosensory dysfunction prior to testing for the presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in patients attending a COVID-19 screening facility.
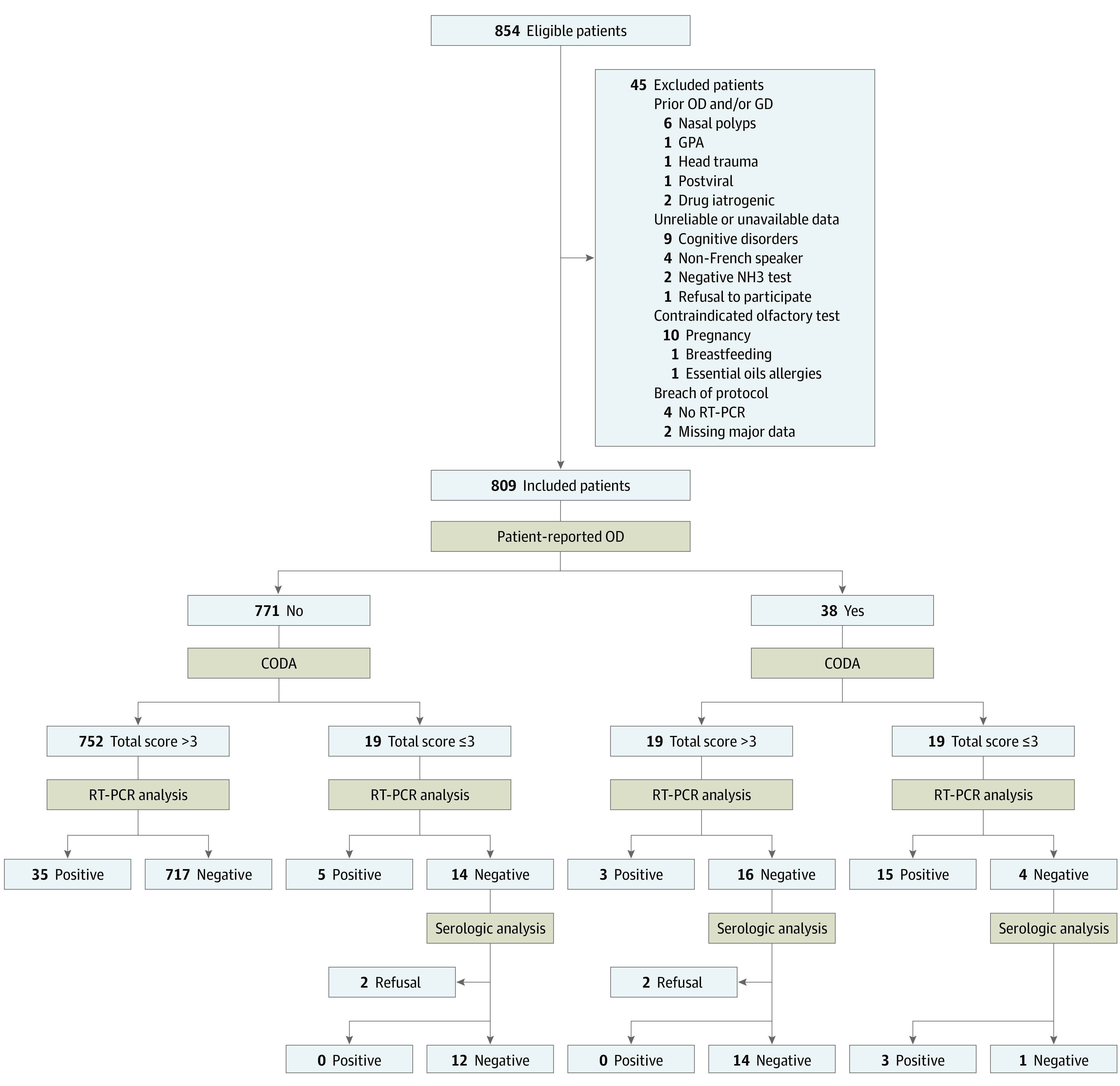
Design, setting, and participants: This prospective diagnostic study with participants and observers blinded to COVID-19 status was conducted in a COVID-19 screening center of a tertiary university hospital in France from March 23 to April 22, 2020. Participants were 854 consecutively included health care workers or outpatients with symptoms or with close contact with an index case. Exclusion criteria were prior chemosensory dysfunction, testing inability, or contraindications (n = 45).
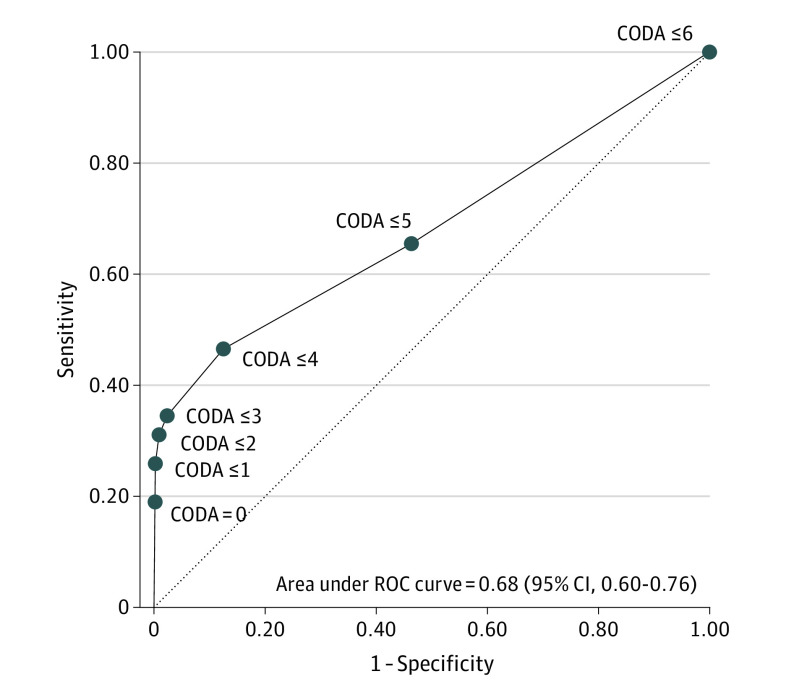
Main outcomes and measures: Participants were interviewed to ascertain their symptoms and then underwent Clinical Olfactory Dysfunction Assessment (CODA), an ad hoc test developed for a simple and fast evaluation of olfactory function. This assessment followed a standardized procedure in which participants identified and rated the intensity of 3 scents (lavender, lemongrass, and mint) to achieve a summed score ranging from 0 to 6. The COVID-19 status was assessed using reverse transcriptase-polymerase chain reaction to detect the presence of SARS-CoV-2 in samples collected via nasopharyngeal swab (reference standard) to calculate the diagnostic values of patient-reported chemosensory dysfunction and CODA.
Results: Of 809 participants, the female to male sex ratio was 2.8, and the mean (SD) age was 41.8 (13.0) years (range, 18-94 years). All participants, if symptomatic, had mild disease at the time of testing, and 58 (7.2%) tested positive for SARS-CoV-2. Chemosensory dysfunction was reported by 20 of 58 participants (34.5%) with confirmed COVID-19 vs 29 of 751 participants (3.9%) who tested negative for COVID-19 (absolute difference, 30.6% [95% CI, 18.3%-42.9%]). Olfactory dysfunction, either self-reported or clinically ascertained (CODA score ≤3), yielded similar sensitivity (0.31 [95% CI, 0.20-0.45] vs 0.34 [95% CI, 0.22-0.48]) and specificity (0.97 [95% CI, 0.96-0.98) vs 0.98 [95% CI, 0.96-0.99]) for COVID-19 diagnosis. Concordance was high between reported and clinically tested olfactory dysfunction, with a Gwet AC1 of 0.95 (95% CI, 0.93-0.97). Of 19 participants, 15 (78.9%) with both reported olfactory dysfunction and a CODA score of 3 or lower were confirmed to have COVID-19. The CODA score also revealed 5 of 19 participants (26.3%) with confirmed COVID-19 who had previously unperceived olfactory dysfunction.
Conclusions and relevance: In this prospective diagnostic study of outpatients with asymptomatic or mild to moderate COVID-19, systematically assessed anamnesis and clinical testing with the newly developed CODA were complementary and specific for chemosensory dysfunction. Olfactory dysfunction was suggestive of COVID-19, particularly when clinical testing confirmed anamnesis. However, normal olfaction was most common among patients with COVID-19.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
