

Transbronchial biopsies' histopathological findings leading to successful late steroid therapy in Covid-19 acute respiratory failure
- PMID: 33411031
- PMCID: PMC7789084
- DOI: 10.1007/s00428-020-02975-6
Transbronchial biopsies' histopathological findings leading to successful late steroid therapy in Covid-19 acute respiratory failure
Abstract
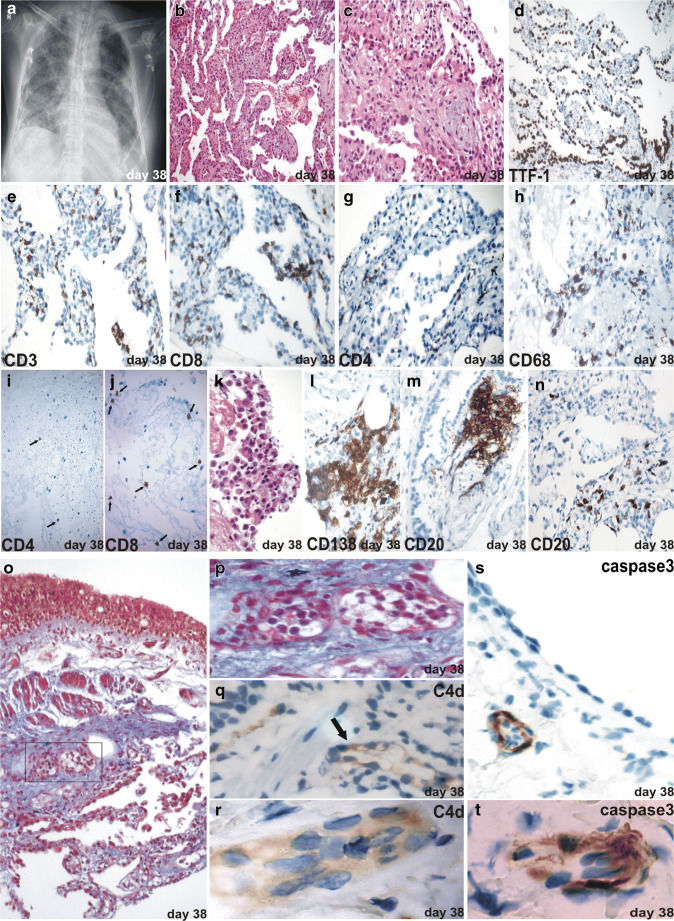
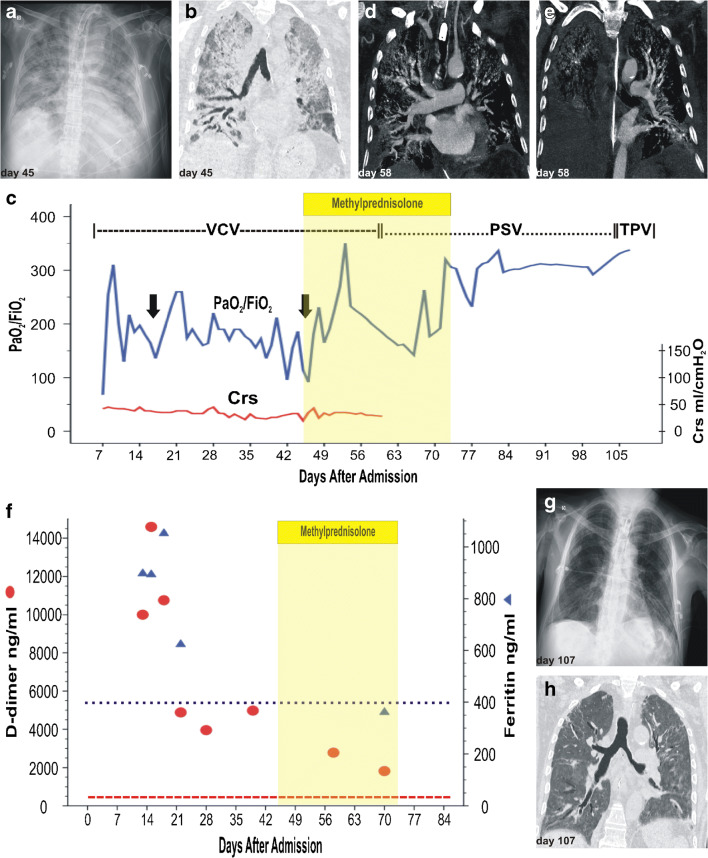
We present results from clinical, radiologic, gas exchange, lung mechanics, and fibre-optic bronchoscopy-guided transbronchial biopsies in a case of acute respiratory failure due to SARS-CoV-2 (Covid-19). This report highlights the pulmonary, immunological, and inflammatory changes found during acute diffuse alveolar damage and the later organizing phase. An early diffuse alveolar damage pattern with predominant epithelial involvement with active recruitment of T cells and monocytes was observed followed by a late organizing pattern with pneumocyte hyperplasia, inflammatory infiltration, prominent endotheliitis, and secondary germinal centers. The patient's deterioration paralleling the late immuno-pathological findings based the decision to administer intravenous corticosteroids, resulting in clinical, gasometric, and radiologic improvement. We believe that real-time clinicopathological correlation, along with the description of the immunological processes at play, will contribute to the full clinical picture of Covid-19 and might lead to a more rational approach in the precise timing of anti-inflammatory, anti-cytokine, or steroid therapies.
Keywords: Acute respiratory failure; Covid-19; Lung histology; Pathology; SARS-CoV-2; Transbronchial biopsy.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Ministerio de Salud, Argentina (2020) nuevo-coronavirus-covid-19-reporte-diario. https://www.argentina.gob.ar/coronavirus/informe-diario. Accessed 26 July 2020
-
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi: 10.1001/jama.2020.1585. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
