

Quantitative analysis of dynamic computed tomography angiography for the detection of endoleaks after abdominal aorta aneurysm endovascular repair: A feasibility study
- PMID: 33411747
- PMCID: PMC7790279
- DOI: 10.1371/journal.pone.0245134
Quantitative analysis of dynamic computed tomography angiography for the detection of endoleaks after abdominal aorta aneurysm endovascular repair: A feasibility study
Abstract
Objectives: To assess the feasibility of quantitative analysis of dynamic computed tomography angiography (dCTA) for the detection of endoleaks in patients who underwent endovascular repair of abdominal aortic aneurysms (EVAR).
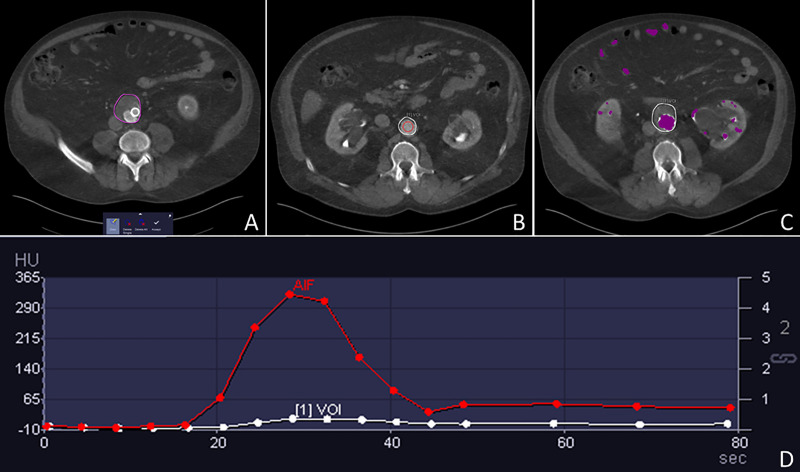
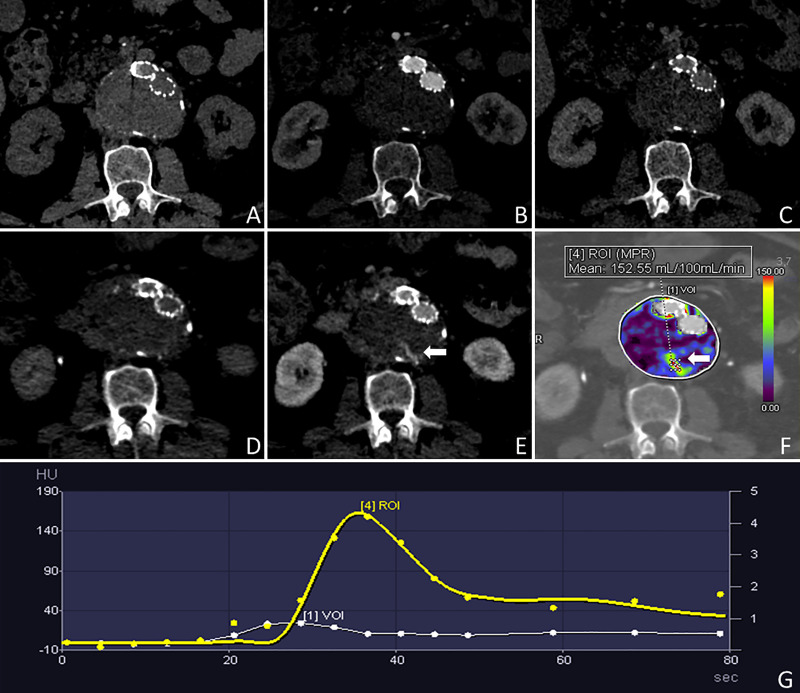
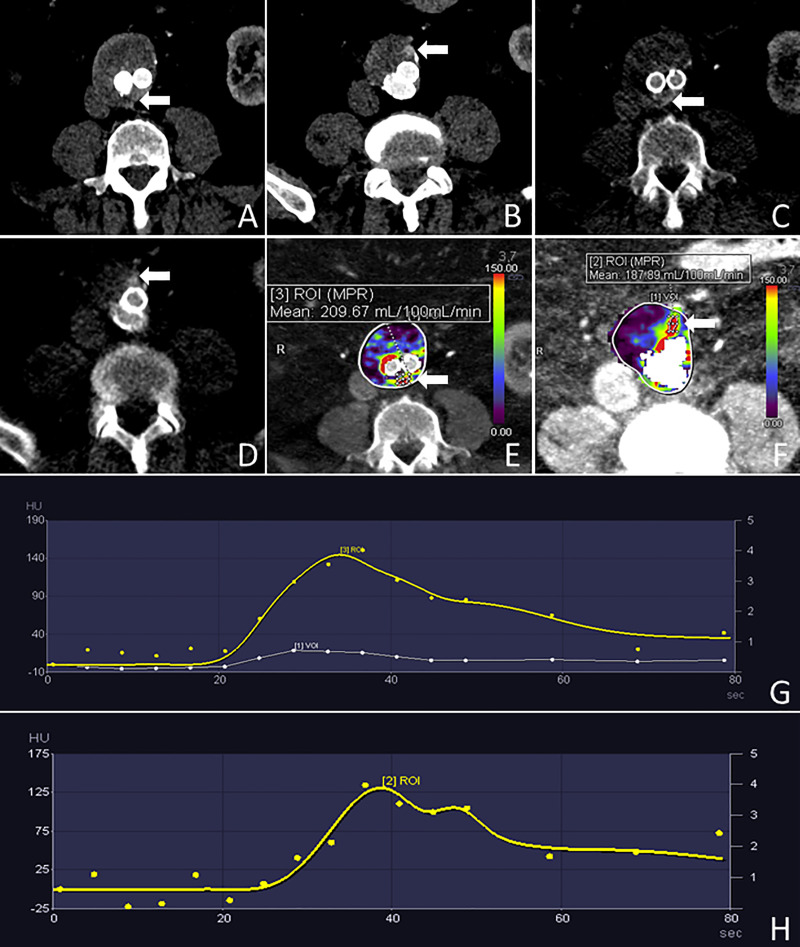
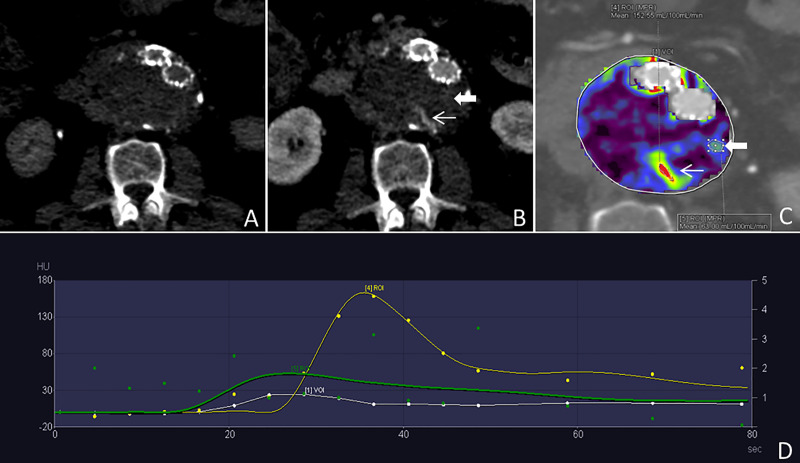
Material and methods: Twenty patients scheduled for contrast-enhanced CT angiography (CTA) of the abdominal aorta post-EVAR were prospectively enrolled. All patients received a standard triphasic CTA protocol, followed by an additional dCTA. The dCTA acquisition enabled reconstruction of color-coded maps depicting blood perfusion and a dCTA dataset of the aneurysm sac. Observers assessed the dCTA and dynamic CT perfusion (dCTP) images for the detection of endoleaks, establishing diagnostic confidence based on a modified 5-point Likert scale. An index was calculated for the ratio between the endoleak and aneurysm sac using blood flow for dCTP and Hounsfield units (HU) for dCTA. The Wilcoxon test compared the endoleak index and the diagnostic confidence of the observers.
Results: In total, 19 patients (18 males, median age 74 years [70.5-75.7]) were included for analysis. Nine endoleaks were detected in 7 patients using triphasic CTA as the reference standard. There was complete agreement for endoleak detection between the two techniques on a per-patient basis. Both dCTA and dCTP identified an additional endoleak in one patient. The diagnostic confidence using dCTP for detection of endoleaks was not significantly superior to dCTA (5.0 [5-5] vs. 4.5 [4-5], respectively; p = 0.11); however, dCTP demonstrated superior diagnostic confidence for endoleak exclusion compared to dCTA (1.0 [1-1] vs 1.5 [1.5-1.5], respectively; p <0.01). Moreover, the dCTP endoleak index was significantly higher than the dCTA index (18.5 [10.8-20.5] vs. 3.5 [5-2.7], respectively; p = 0.02).
Conclusions: Quantitative analysis of dCTP imaging can aid in the detection of endoleaks and demonstrates a higher endoleak detection rate than triphasic CTA, as well as a strong correlation with visual assessment of dCTA images.
Conflict of interest statement
Dr. Schoepf receives institutional research support from and is a consultant for Bayer, Bracco, Elucid Bioimaging, Guerbet, HeartFlow, and Siemens. Dr. Varga-Szemes receives institutional research support from Siemens and is a consultant for Bayer and Elucid Bioimaging. The other authors have no conflict of interest to disclose. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Dynamic Computed Tomography Angiography as Imaging Method for Endoleak Classification after Endovascular Aneurysm Repair: A Case Series and Systematic Review of the Literature.Diagnostics (Basel). 2023 Feb 21;13(5):829. doi: 10.3390/diagnostics13050829. Diagnostics (Basel). 2023. PMID: 36899973 Free PMC article. Review.
-
The Role of Dynamic Computed Tomography Angiography in Endoleak Detection and Classification After Endovascular Aneurysm Repair: A Comprehensive Review.Diagnostics (Basel). 2025 Feb 4;15(3):370. doi: 10.3390/diagnostics15030370. Diagnostics (Basel). 2025. PMID: 39941300 Free PMC article. Review.
-
Detection of Endoleaks Following Thoracic and Abdominal Aortic Endovascular Aortic Repair-: A Comparison of Standard and Dynamic 4D-Computed Tomography Angiography.J Endovasc Ther. 2023 Oct;30(5):739-745. doi: 10.1177/15266028221095390. Epub 2022 May 18. J Endovasc Ther. 2023. PMID: 35582987
-
Feasibility of shear wave sonoelastography to detect endoleak and evaluate thrombus organization after endovascular repair of abdominal aortic aneurysm.Eur Radiol. 2020 Jul;30(7):3879-3889. doi: 10.1007/s00330-020-06739-3. Epub 2020 Mar 4. Eur Radiol. 2020. PMID: 32130495
-
Dynamic CT angiography after abdominal aortic endovascular aneurysm repair: differences in contrast agent dynamics in the aorta and endoleaks--preliminary results.J Vasc Interv Radiol. 2012 Jun;23(6):744-50. doi: 10.1016/j.jvir.2012.02.008. Epub 2012 Apr 10. J Vasc Interv Radiol. 2012. PMID: 22494657
Cited by
-
Dynamic Computed Tomography Angiography as Imaging Method for Endoleak Classification after Endovascular Aneurysm Repair: A Case Series and Systematic Review of the Literature.Diagnostics (Basel). 2023 Feb 21;13(5):829. doi: 10.3390/diagnostics13050829. Diagnostics (Basel). 2023. PMID: 36899973 Free PMC article. Review.
-
Accuracy Verification of Four-Dimensional CT Analysis of Knee Joint Movements: A Pilot Study Using a Knee Joint Model and Motion-Capture System.Cureus. 2023 Feb 28;15(2):e35616. doi: 10.7759/cureus.35616. eCollection 2023 Feb. Cureus. 2023. PMID: 37007305 Free PMC article.
-
Utility of 4D CT in endoleak characterization after advanced endovascular aortic repair.Vascular. 2023 Dec;31(6):1069-1075. doi: 10.1177/17085381221105326. Epub 2022 Jun 2. Vascular. 2023. PMID: 35652274 Free PMC article.
-
The Role of Dynamic Computed Tomography Angiography in Endoleak Detection and Classification After Endovascular Aneurysm Repair: A Comprehensive Review.Diagnostics (Basel). 2025 Feb 4;15(3):370. doi: 10.3390/diagnostics15030370. Diagnostics (Basel). 2025. PMID: 39941300 Free PMC article. Review.
-
EVAR Follow-Up with Ultrasound Superb Microvascular Imaging (SMI) Compared to CEUS and CT Angiography for Detection of Type II Endoleak.Diagnostics (Basel). 2022 Feb 18;12(2):526. doi: 10.3390/diagnostics12020526. Diagnostics (Basel). 2022. PMID: 35204615 Free PMC article.
References
-
- Columbo J.A., Kang R., Hoel A.W., Kang J., Leinweber K.A., Tauber K.S., et al., A comparison of reintervention rates after endovascular aneurysm repair between the Vascular Quality Initiative registry, Medicare claims, and chart review. J Vasc Surg, 2019;69(1):74–79 e6. 10.1016/j.jvs.2018.03.423 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
