

Hospital-based evidence on cost-effectiveness of brucellosis diagnostic tests and treatment in Kenyan hospitals
- PMID: 33411798
- PMCID: PMC7833147
- DOI: 10.1371/journal.pntd.0008977
Hospital-based evidence on cost-effectiveness of brucellosis diagnostic tests and treatment in Kenyan hospitals
Abstract
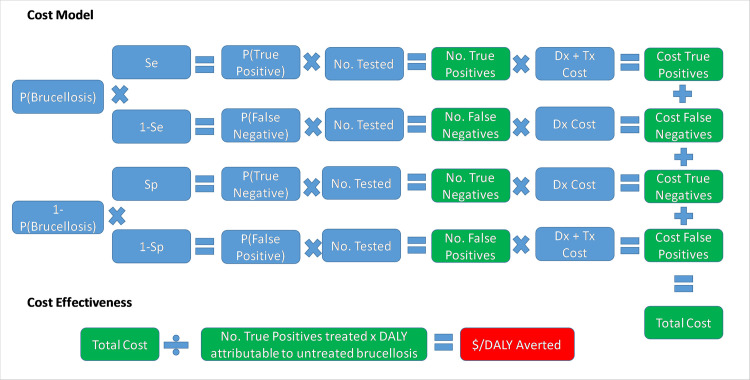
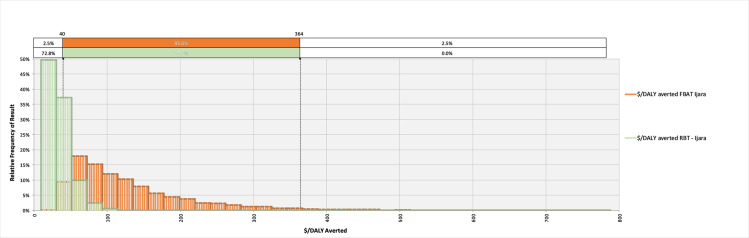
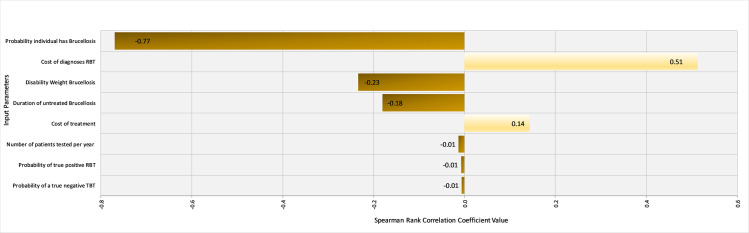
Hospitals in Kenya continue to use the Febrile Antigen Brucella Agglutination Test (FBAT) to diagnose brucellosis, despite reports showing its inadequacy. This study generated hospital-based evidence on the performance and cost-effectiveness of the FBAT, compared to the Rose Bengal Test (RBT).Twelve hospitals in western Kenya stored patient serum samples that were tested for brucellosis using the FBAT, and these were later re-tested using the RBT. Data on the running time and cost of the FBAT, and the treatment prescribed for brucellosis, were collected. The cost-effectiveness of the two tests, defined as the cost in US Dollars ($) per Disability Adjusted Life Year (DALY) averted, was determined, and a basic sensitivity analysis was run to identify the most influential parameters. Over a 6-month period, 180 patient serum samples that were tested with FBAT at the hospitals were later re-tested with RBT at the field laboratory. Of these 24 (13.3%) and 3 (1.7%) tested positive with FBAT and RBT, respectively. The agreement between the FBAT and RBT was slight (Kappa = 0.12). Treatment prescribed following FBAT positivity varied between hospitals, and only one hospital prescribed a standardized therapy regimen. The mean $/DALY averted when using the FBAT and RBT were $2,065 (95% CI $481-$6,736) and $304 (95% CI $126-$604), respectively. Brucellosis prevalence was the most influential parameter in the cost-effectiveness of both tests. Extrapolation to the national level suggested that an estimated $338,891 (95% CI $47,000-$1,149,000) per year is currently spent unnecessarily treating those falsely testing positive by FBAT. These findings highlight the potential for misdiagnosis using the FBAT. Furthermore, the RBT is cost-effective, and could be considered as the mainstay screening test for human brucellosis in this setting. Lastly, the treatment regimens must be harmonized to ensure the appropriate use of antibiotics for treatment.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures



References
-
- World Health Organization. The control of neglected zoonotic diseases: from advocacy to action: report of the fourth international meeting held at WHO Headquarters, Geneva, Switzerland, 19–20 November 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/183458/9789241508568_en....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
