

COVID-19-neutralizing antibodies predict disease severity and survival
- PMID: 33412089
- PMCID: PMC7837114
- DOI: 10.1016/j.cell.2020.12.015
COVID-19-neutralizing antibodies predict disease severity and survival
Abstract
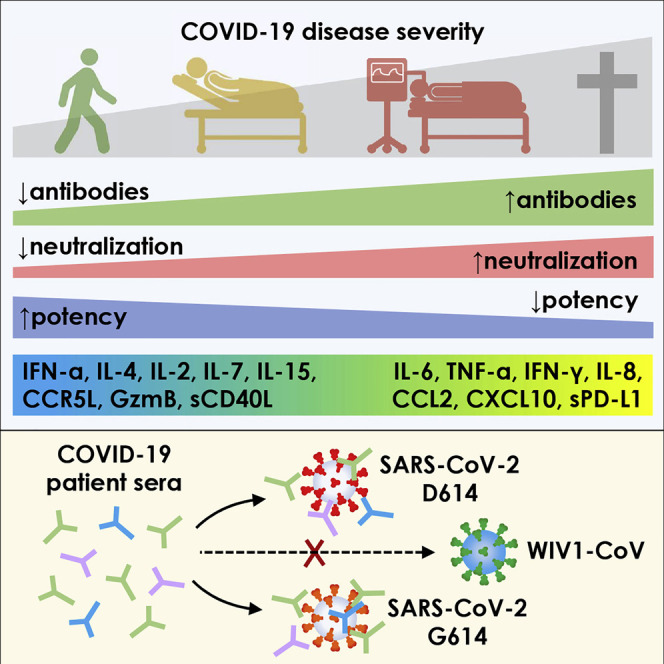
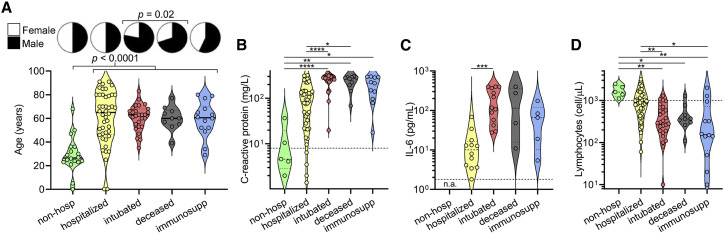
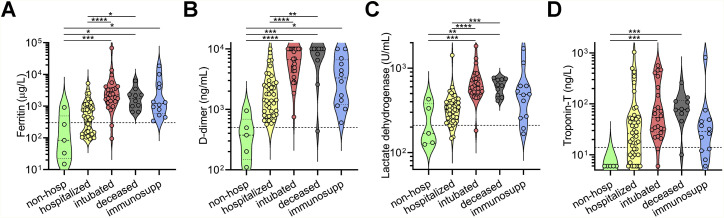
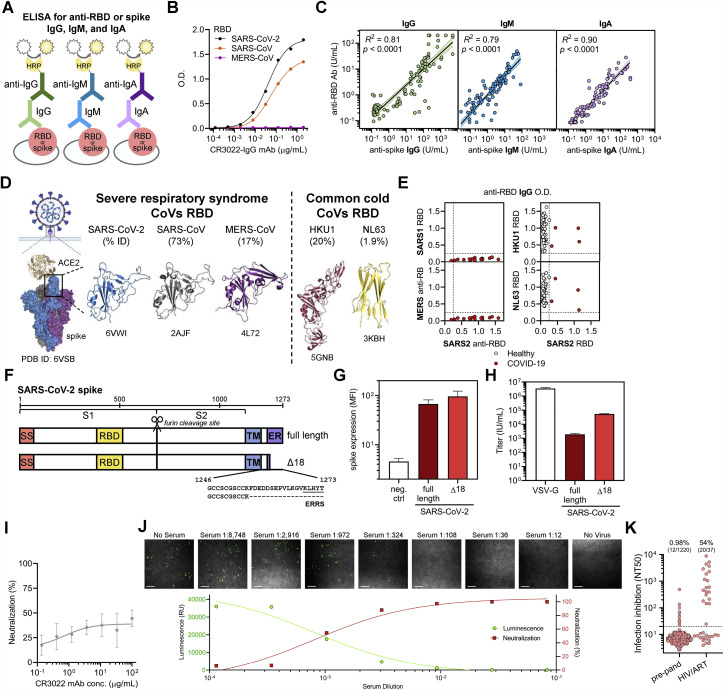
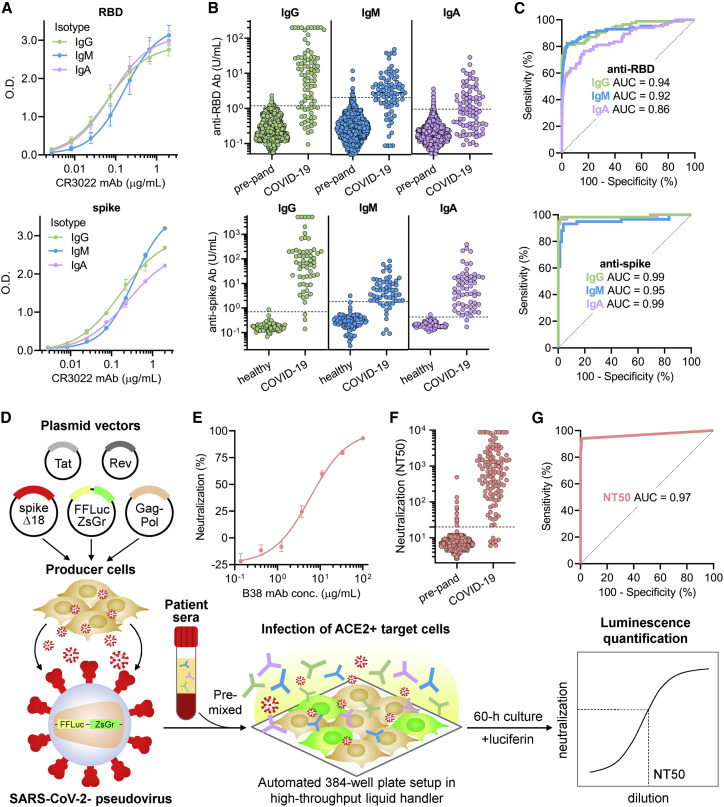
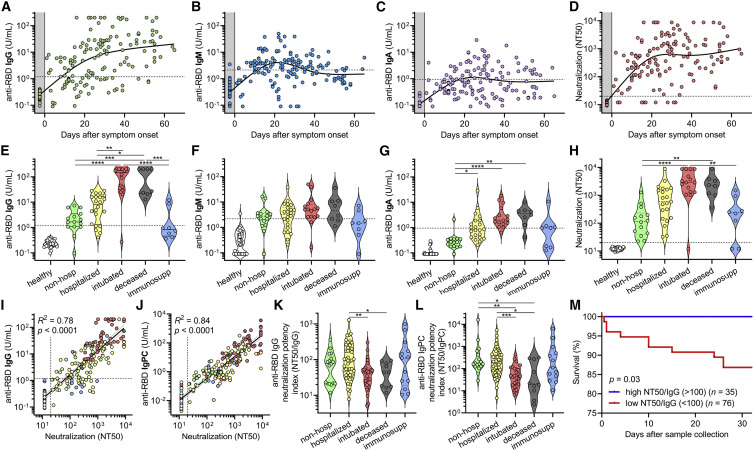
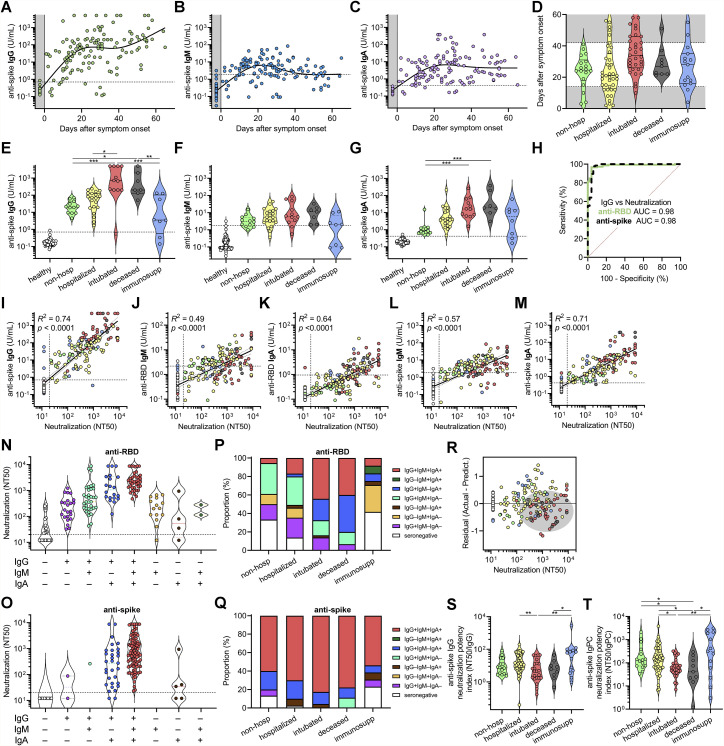
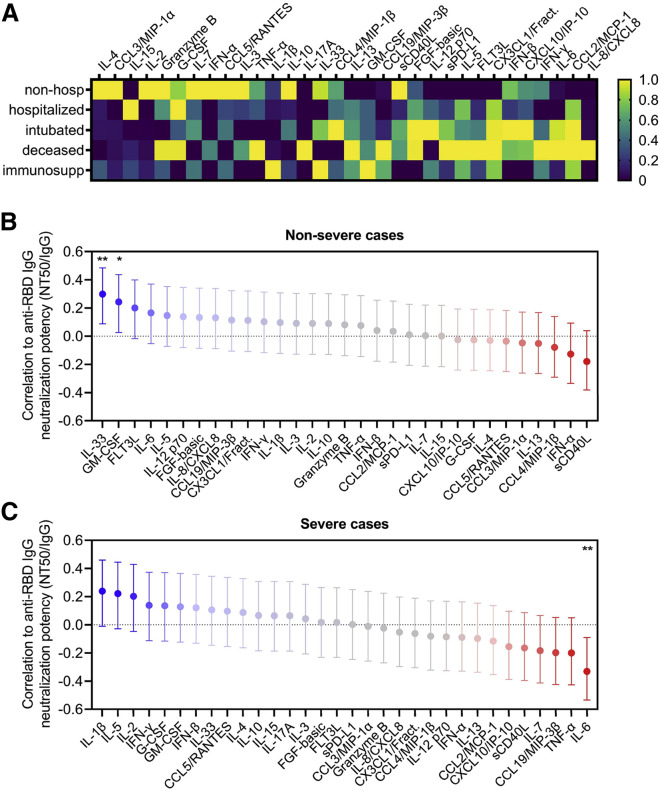
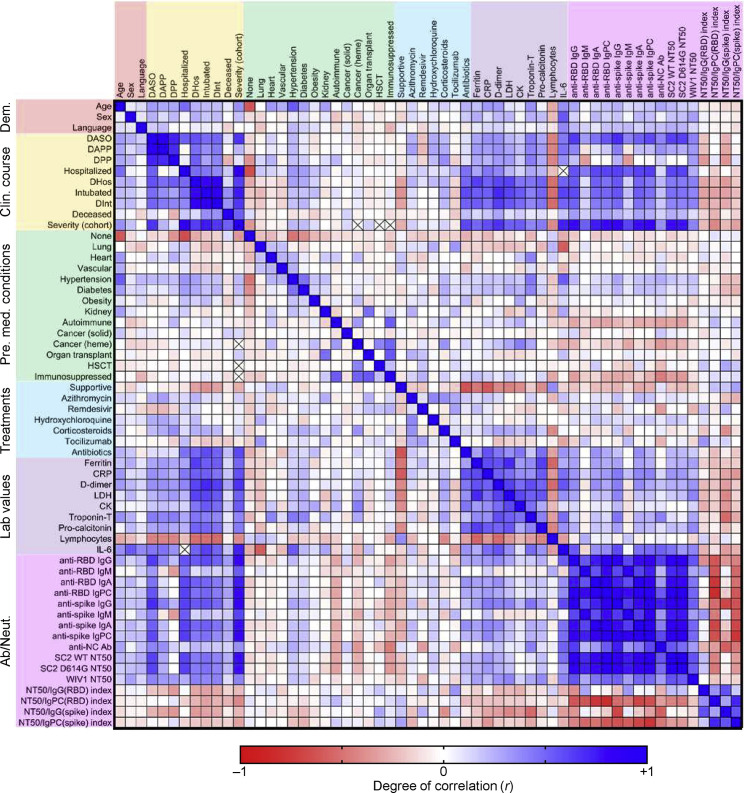
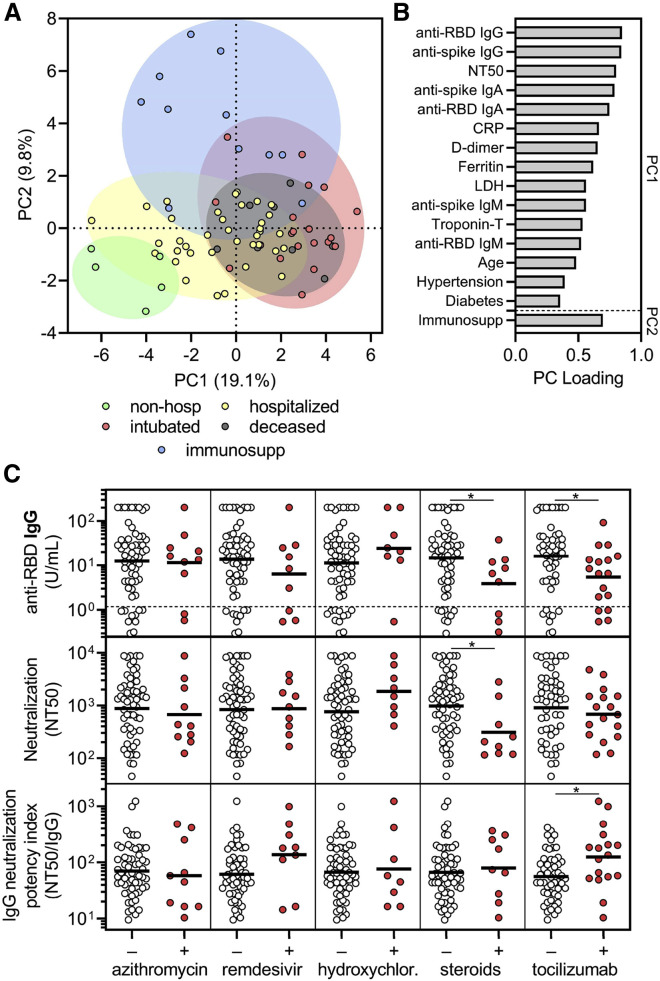
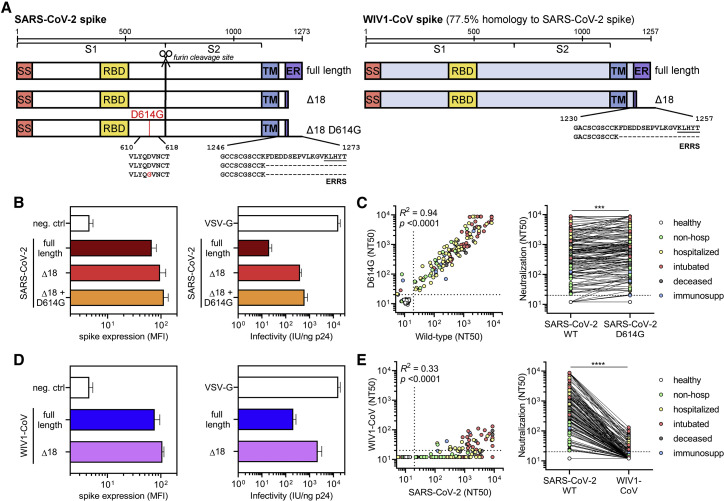
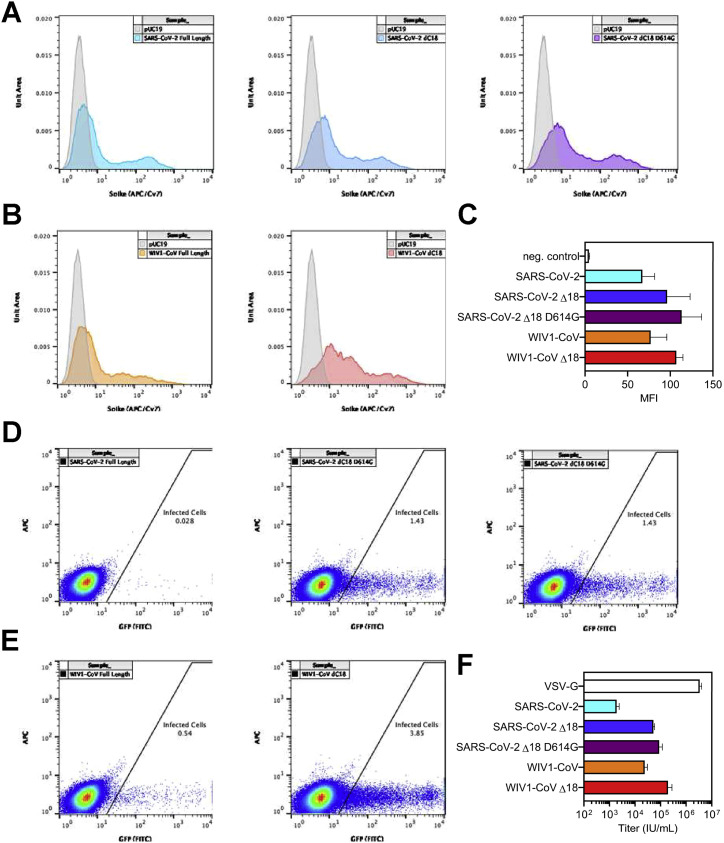
Coronavirus disease 2019 (COVID-19) exhibits variable symptom severity ranging from asymptomatic to life-threatening, yet the relationship between severity and the humoral immune response is poorly understood. We examined antibody responses in 113 COVID-19 patients and found that severe cases resulting in intubation or death exhibited increased inflammatory markers, lymphopenia, pro-inflammatory cytokines, and high anti-receptor binding domain (RBD) antibody levels. Although anti-RBD immunoglobulin G (IgG) levels generally correlated with neutralization titer, quantitation of neutralization potency revealed that high potency was a predictor of survival. In addition to neutralization of wild-type SARS-CoV-2, patient sera were also able to neutralize the recently emerged SARS-CoV-2 mutant D614G, suggesting cross-protection from reinfection by either strain. However, SARS-CoV-2 sera generally lacked cross-neutralization to a highly homologous pre-emergent bat coronavirus, WIV1-CoV, which has not yet crossed the species barrier. These results highlight the importance of neutralizing humoral immunity on disease progression and the need to develop broadly protective interventions to prevent future coronavirus pandemics.
Keywords: COVID-19; D614G; ELISA; RBD; SARS-CoV-2; WIV1-CoV; disease severity; neutralizing antibodies; pro-inflammatory cytokines; spike.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests J.A.B. has served as a paid consultant to T2 Biosystems, DiaSorin, and Roche Diagnostics.
Figures
Update of
-
COVID-19 neutralizing antibodies predict disease severity and survival.medRxiv [Preprint]. 2020 Oct 20:2020.10.15.20213512. doi: 10.1101/2020.10.15.20213512. medRxiv. 2020. Update in: Cell. 2021 Jan 21;184(2):476-488.e11. doi: 10.1016/j.cell.2020.12.015. PMID: 33106822 Free PMC article. Updated. Preprint.
References
-
- Arvin A.M., Fink K., Schmid M.A., Cathcart A., Spreafico R., Havenar-Daughton C., Lanzavecchia A., Corti D., Virgin H.W. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature. 2020;584:353–363. - PubMed
-
- Beigel J.H., Tomashek K.M., Dodd L.E. Remdesivir for the Treatment of Covid-19 - Preliminary Report. Reply. N. Engl. J. Med. 2020;383:994. - PubMed
-
- Chan K.H., Cheng V.C.C., Woo P.C.Y., Lau S.K.P., Poon L.L.M., Guan Y., Seto W.H., Yuen K.Y., Peiris J.S.M. Serological responses in patients with severe acute respiratory syndrome coronavirus infection and cross-reactivity with human coronaviruses 229E, OC43, and NL63. Clin. Diagn. Lab. Immunol. 2005;12:1317–1321. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AI153098/AI/NIAID NIH HHS/United States
- R01 AI155447/AI/NIAID NIH HHS/United States
- T32 AI007245/AI/NIAID NIH HHS/United States
- T32 GM007753/GM/NIGMS NIH HHS/United States
- F32 AI143480/AI/NIAID NIH HHS/United States
- R01 AI146779/AI/NIAID NIH HHS/United States
- DP2 DA040254/DA/NIDA NIH HHS/United States
- DP2 DA042422/DA/NIDA NIH HHS/United States
- T32 GM008313/GM/NIGMS NIH HHS/United States
- R01 AI124378/AI/NIAID NIH HHS/United States
- R21 AI119457/AI/NIAID NIH HHS/United States
- R01 AI137057/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
