

Cardiovascular risk factors and mortality in hospitalized patients with COVID-19: systematic review and meta-analysis of 45 studies and 18,300 patients
- PMID: 33413093
- PMCID: PMC7789083
- DOI: 10.1186/s12872-020-01816-3
Cardiovascular risk factors and mortality in hospitalized patients with COVID-19: systematic review and meta-analysis of 45 studies and 18,300 patients
Abstract
Background: A high prevalence of cardiovascular risk factors including age, male sex, hypertension, diabetes, and tobacco use, has been reported in patients with Coronavirus disease 2019 (COVID-19) who experienced adverse outcome. The aim of this study was to investigate the relationship between cardiovascular risk factors and in-hospital mortality in patients with COVID-19.
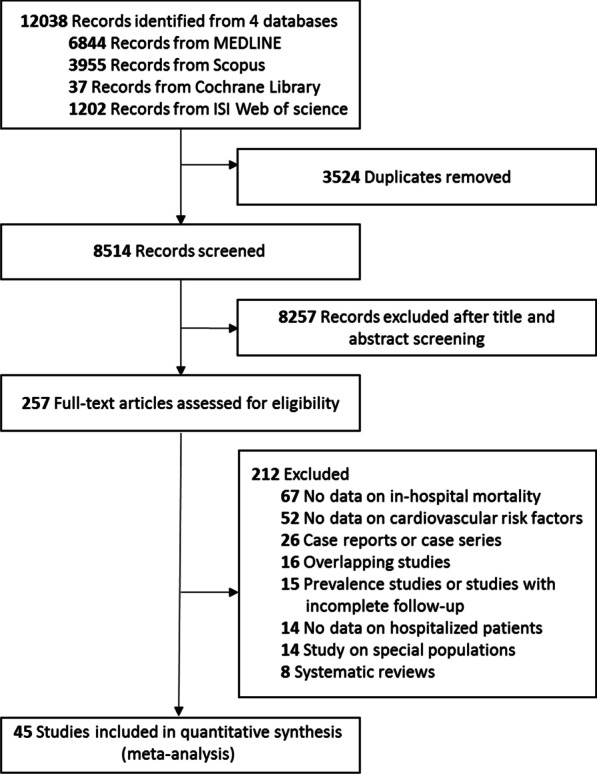
Methods: MEDLINE, Cochrane, Web of Sciences, and SCOPUS were searched for retrospective or prospective observational studies reporting data on cardiovascular risk factors and in-hospital mortality in patients with COVID-19. Univariable and multivariable age-adjusted analyses were conducted to evaluate the association between cardiovascular risk factors and the occurrence of in-hospital death.
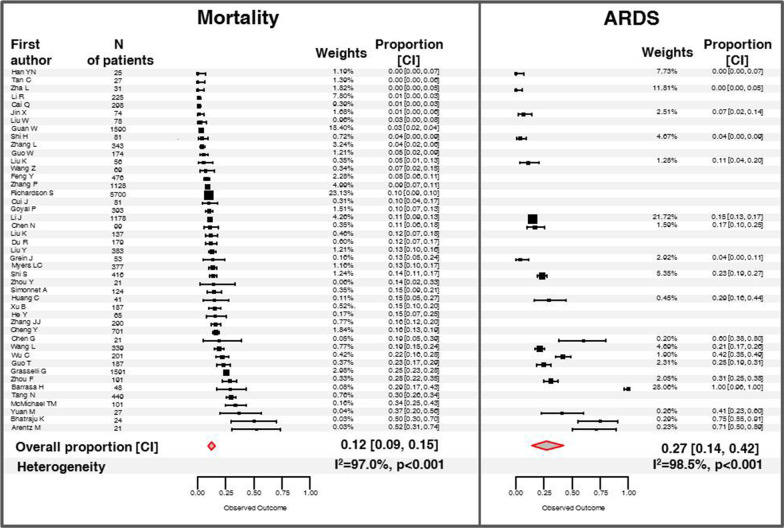
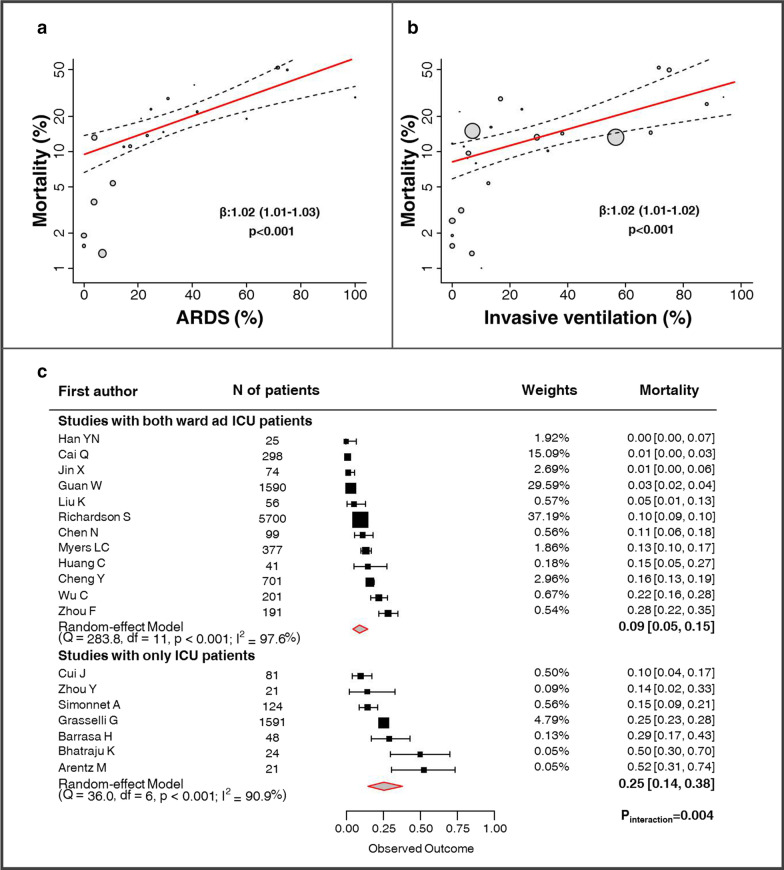
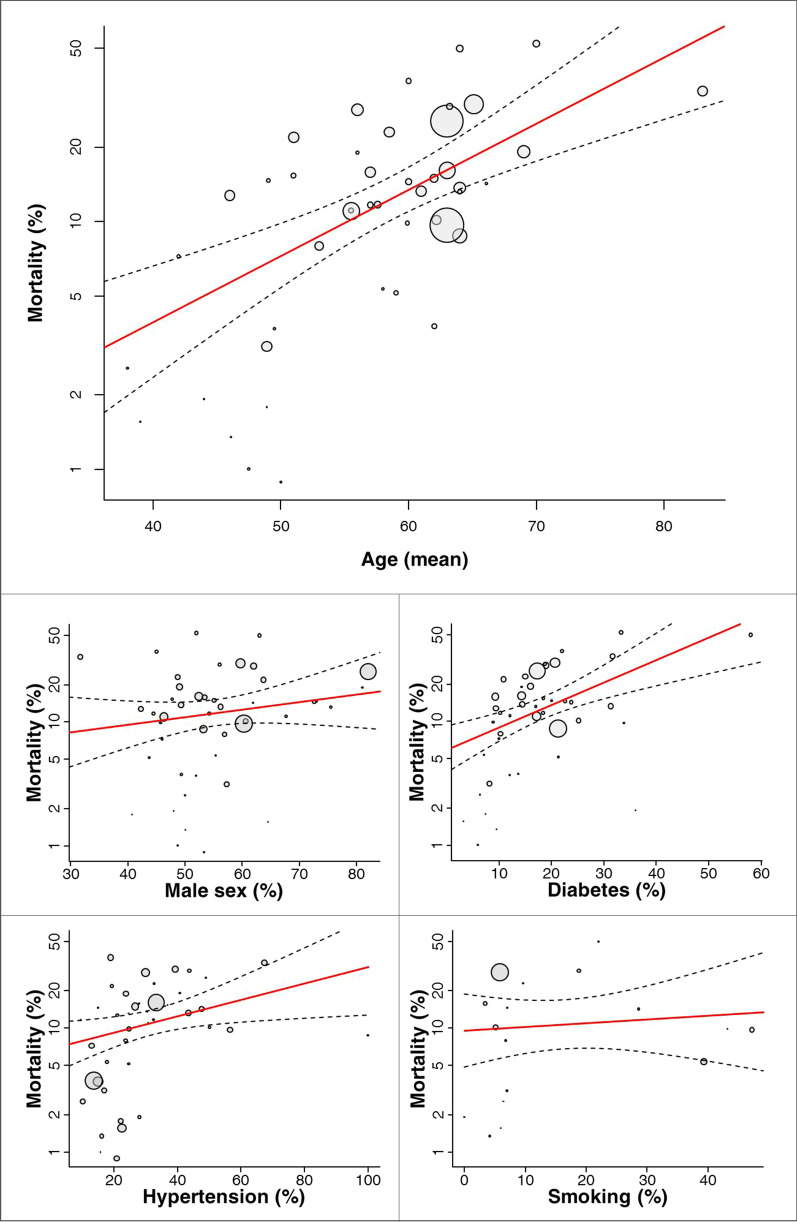
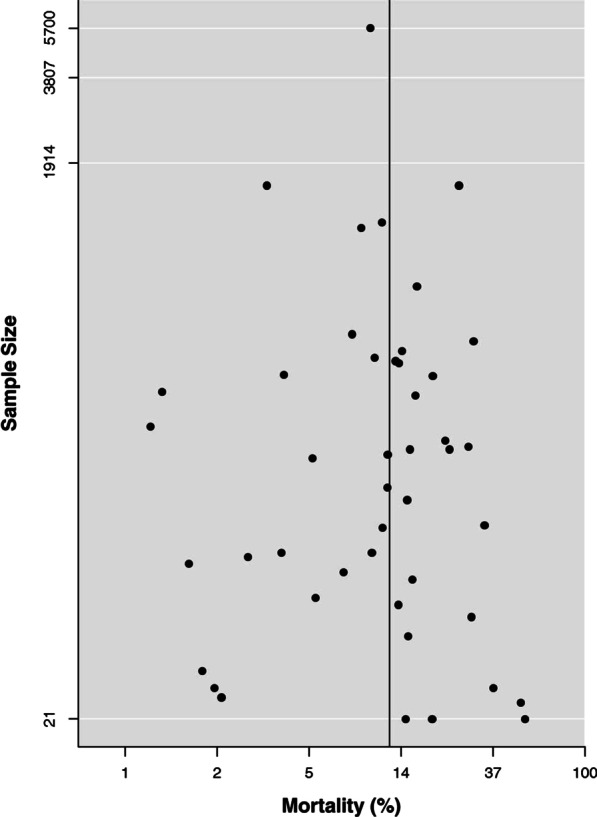
Results: The analysis included 45 studies enrolling 18,300 patients. The pooled estimate of in-hospital mortality was 12% (95% CI 9-15%). The univariable meta-regression analysis showed a significant association between age (coefficient: 1.06; 95% CI 1.04-1.09; p < 0.001), diabetes (coefficient: 1.04; 95% CI 1.02-1.07; p < 0.001) and hypertension (coefficient: 1.01; 95% CI 1.01-1.03; p = 0.013) with in-hospital death. Male sex and smoking did not significantly affect mortality. At multivariable age-adjusted meta-regression analysis, diabetes was significantly associated with in-hospital mortality (coefficient: 1.02; 95% CI 1.01-1.05; p = 0.043); conversely, hypertension was no longer significant after adjustment for age (coefficient: 1.00; 95% CI 0.99-1.01; p = 0.820). A significant association between age and in-hospital mortality was confirmed in all multivariable models.
Conclusions: This meta-analysis suggests that older age and diabetes are associated with higher risk of in-hospital mortality in patients infected by SARS-CoV-2. Conversely, male sex, hypertension, and smoking did not independently correlate with fatal outcome.
Keywords: COVID-19; Cardiovascular risk factors; Diabetes; Hypertension; Mortality; Novel coronavirus; Outcome; SARS-CoV-2; Smoking.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Cook DJ, Marshall JC, Fowler RA. Critical illness in patients with COVID-19: mounting an effective clinical and research response. Jama. 2020 [Epub ahead of print]. - PubMed
-
- World Health Organization Coronavirus disease 2019 (COVID-19). Situation Report—141. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 10 June 2020.
-
- Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. Jama. 2020 [Epub ahead of print]. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
