

Assessing responsiveness of the EQ-5D-3L, the Oxford Hip Score, and the Oxford Knee Score in the NHS patient-reported outcome measures
- PMID: 33413483
- PMCID: PMC7791983
- DOI: 10.1186/s13018-020-02126-2
Assessing responsiveness of the EQ-5D-3L, the Oxford Hip Score, and the Oxford Knee Score in the NHS patient-reported outcome measures
Erratum in
-
Correction to: Assessing responsiveness of the EQ-5D-3L, the Oxford Hip Score, and the Oxford Knee Score in the NHS patient-reported outcome measures.J Orthop Surg Res. 2021 Feb 5;16(1):115. doi: 10.1186/s13018-021-02273-0. J Orthop Surg Res. 2021. PMID: 33546672 Free PMC article. No abstract available.
Abstract
Background: The degree to which a validated instrument is able to detect clinically significant change over time is an important issue for the better management of hip or knee replacement surgery. This study examines the internal responsiveness of the EQ-5D-3L, the Oxford Hip Score (OHS), and the Oxford Knee Score (OKS) by various methods. Data from NHS patient-reported outcome measures (PROMs) linked to the Hospital Episodes Statistics (HES) dataset (2009-2015) was analysed for patients who underwent primary hip surgery (N = 181,424) and primary knee surgery (N = 191,379).
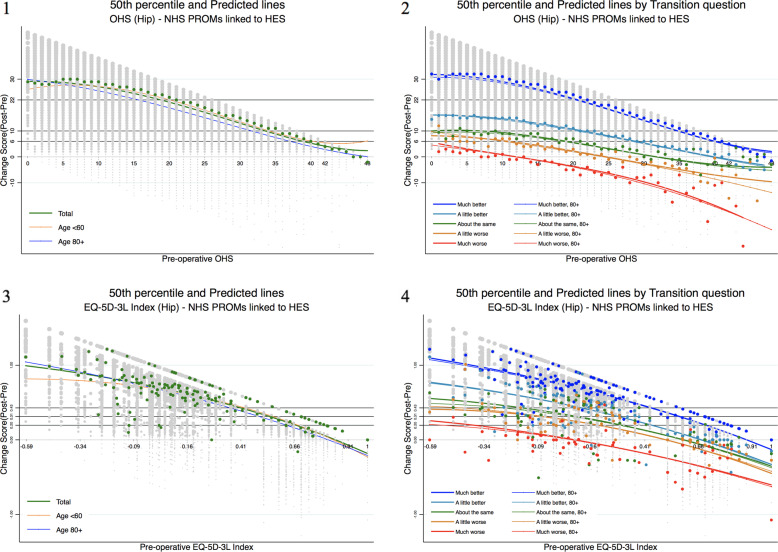
Methods: Paired data-specific univariate responsiveness was investigated using the standardized response mean (SRM), the standardized effect size (SES), and the responsiveness index (RI). Multivariate responsiveness was furthermore examined using the defined capacity of benefit score (i.e. paired data-specific MCID), adjusting baseline covariates such as age, gender, and comorbidities in the Box-Cox regression models. The observed and predicted percentages of patient improvement were examined both as a whole and by the patients' self-assessed transition level.
Results: The results showed that both the OHS and the OKS demonstrated great univariate and multivariate responsiveness. The percentages of the observed (predicted) total improvement were high: 51 (54)% in the OHS and 73 (58)% in OKS. The OHS and the OKS showed distinctive differences in improvement by the 3-level transition, i.e. a little better vs. about the same vs. a little worse. The univariate responsiveness of the EQ-5D-3L showed moderate effects in total by Cohen's thresholds. The percentages of improvement in the EQ-5D-3L were moderate: 44 (48)% in the hip and 42 (44)% for the knee replacement population.
Conclusions: Distinctive percentage differences in patients' perception of improvement were observed when the paired data-specific capacity of benefit score was applied to examine responsiveness. This is useful in clinical practice as rationale for access to surgery at the individual-patient level. This study shows the importance of analytic methods and instruments for investigation of the health status in hip and/or knee replacement surgery. The study finding also supports the idea of using a generic measure along with the disease-specific instruments in terms of cross-validation.
Keywords: EQ-5D-3L Index; Hip and knee replacement; Internal responsiveness; OHS; OKS; Patient-reported outcome.
Conflict of interest statement
There are no conflicts of interest to disclose regarding any financial or personal relationship.
Figures
Similar articles
-
Socioeconomic inequalities in patient-reported outcome measures among total hip and knee arthroplasty patients: a comprehensive analysis of instruments and domains.Int J Equity Health. 2025 May 23;24(1):147. doi: 10.1186/s12939-025-02520-4. Int J Equity Health. 2025. PMID: 40410867 Free PMC article.
-
The Arthroplasty Candidacy Help Engine tool to select candidates for hip and knee replacement surgery: development and economic modelling.Health Technol Assess. 2019 Jun;23(32):1-216. doi: 10.3310/hta23320. Health Technol Assess. 2019. PMID: 31287051 Free PMC article.
-
Associations between preoperative Oxford hip and knee scores and costs and quality of life of patients undergoing primary total joint replacement in the NHS England: an observational study.BMJ Open. 2018 Apr 10;8(4):e019477. doi: 10.1136/bmjopen-2017-019477. BMJ Open. 2018. PMID: 29643154 Free PMC article.
-
How do Patient-reported Outcome Scores in International Hip and Knee Arthroplasty Registries Compare?Clin Orthop Relat Res. 2022 Oct 1;480(10):1884-1896. doi: 10.1097/CORR.0000000000002306. Epub 2022 Jul 8. Clin Orthop Relat Res. 2022. PMID: 35901444 Free PMC article.
-
A systematic review of crosswalks for converting patient-reported outcome measure scores in hip, knee, and shoulder replacement surgery.Acta Orthop. 2024 Sep 13;95:512-523. doi: 10.2340/17453674.2024.41384. Acta Orthop. 2024. PMID: 39268815 Free PMC article.
Cited by
-
Long-Term Outcomes of Primary Cemented Total Hip Arthroplasty with Acetabular Bone Graft for Protrusio Acetabuli: Minimum 10-Year Follow-Up.J Clin Med. 2024 Sep 21;13(18):5612. doi: 10.3390/jcm13185612. J Clin Med. 2024. PMID: 39337099 Free PMC article.
-
Treatment patterns and clinical and economic burden of hip dislocation following primary total hip arthroplasty in England.Bone Joint J. 2022 Jul;104-B(7):811-819. doi: 10.1302/0301-620X.104B7.BJJ-2021-1732.R1. Bone Joint J. 2022. PMID: 35775184 Free PMC article.
-
Evaluation of the EQ-5D-5L, EQ-VAS stand-alone component and Oxford knee score in the Australian knee arthroplasty population utilising minimally important difference, concurrent validity, predictive validity and responsiveness.Health Qual Life Outcomes. 2023 May 10;21(1):41. doi: 10.1186/s12955-023-02126-w. Health Qual Life Outcomes. 2023. PMID: 37165364 Free PMC article.
-
Meaningful values of the EQ-5D-3L in patients undergoing primary knee arthroplasty.Bone Joint Res. 2022 Sep;11(9):619-628. doi: 10.1302/2046-3758.119.BJR-2022-0054.R1. Bone Joint Res. 2022. PMID: 36047008 Free PMC article.
-
Correction to: Assessing responsiveness of the EQ-5D-3L, the Oxford Hip Score, and the Oxford Knee Score in the NHS patient-reported outcome measures.J Orthop Surg Res. 2021 Feb 5;16(1):115. doi: 10.1186/s13018-021-02273-0. J Orthop Surg Res. 2021. PMID: 33546672 Free PMC article. No abstract available.
References
-
- Duncan, P.W., Chapter 9 - Outcome measures in stroke rehabilitation, in Handbook of clinical neurology, M.P. Barnes and D.C. Good, Editors. 2013, Elsevier. p. 105-111. - PubMed
-
- Noyes J, Edwards RT. EQ-5D for the assessment of health-related quality of life and resource allocation in children: a systematic methodological review. Value Health. 2011;14(8):1117–1129. - PubMed
-
- Middel B, van Sonderen E. Statistical significant change versus relevant or important change in (quasi) experimental design: some conceptual and methodological problems in estimating magnitude of intervention-related change in health services research. Int J Integrated Care. 2002;2:e15. - PMC - PubMed
-
- Stewart AL, et al. Functional status and well-being of patients with chronic conditions. Results from the Medical Outcomes Study. Jama. 1989;262(7):907–913. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
