

Cost-effectiveness of a hybrid emergency room system for severe trauma: a health technology assessment from the perspective of the third-party payer in Japan
- PMID: 33413503
- PMCID: PMC7791815
- DOI: 10.1186/s13017-020-00344-x
Cost-effectiveness of a hybrid emergency room system for severe trauma: a health technology assessment from the perspective of the third-party payer in Japan
Abstract
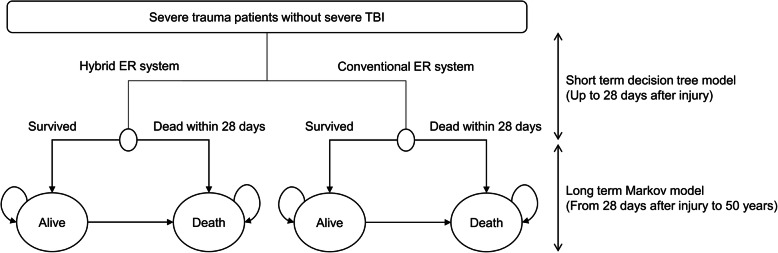
Background: Hybrid emergency room (ER) systems, consisting of an angiography-computed tomography (CT) machine in a trauma resuscitation room, are reported to be effective for reducing death from exsanguination in trauma patients. We aimed to investigate the cost-effectiveness of a hybrid ER system in severe trauma patients without severe traumatic brain injury (TBI).
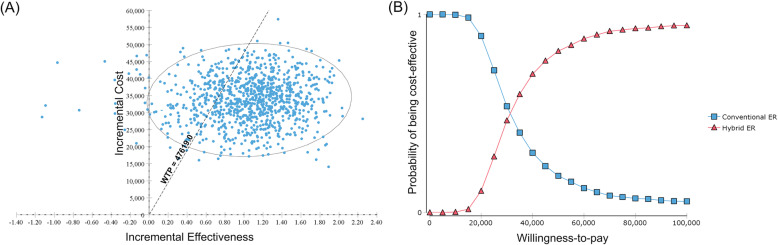
Methods: We conducted a cost-utility analysis comparing the hybrid ER system to the conventional ER system from the perspective of the third-party healthcare payer in Japan. A short-term decision tree and a long-term Markov model using a lifetime time horizon were constructed to estimate quality-adjusted life years (QALYs) and associated lifetime healthcare costs. Short-term mortality and healthcare costs were derived from medical records and claims data in a tertiary care hospital with a hybrid ER. Long-term mortality and utilities were extrapolated from the literature. The willingness-to-pay threshold was set at $47,619 per QALY gained and the discount rate was 2%. Deterministic and probabilistic sensitivity analyses were conducted.
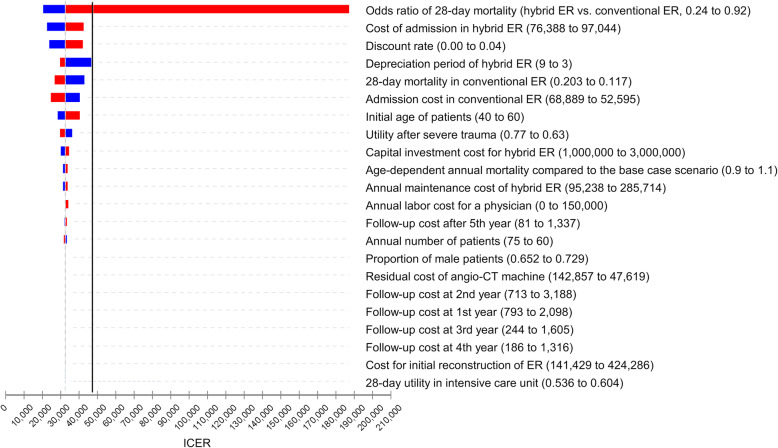
Results: The hybrid ER system was associated with a gain of 1.03 QALYs and an increment of $33,591 lifetime costs compared to the conventional ER system, resulting in an ICER of $32,522 per QALY gained. The ICER was lower than the willingness-to-pay threshold if the odds ratio of 28-day mortality was < 0.66. Probabilistic sensitivity analysis indicated that the hybrid ER system was cost-effective with a 79.3% probability.
Conclusion: The present study suggested that the hybrid ER system is a likely cost-effective strategy for treating severe trauma patients without severe TBI.
Keywords: HERS; ICER; Markov model; QALY; Utility.
Conflict of interest statement
TKinoshita received lecture fees and travel expenses from Canon Medical Systems for lectures given at national and international conferences. TKinoshita was also supported by a Fulbright Japan Graduate Study Program during the conduct of this research. For the remaining authors, no conflicts were declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
