

Invasive lobular carcinoma of the breast: the increasing importance of this special subtype
- PMID: 33413533
- PMCID: PMC7792208
- DOI: 10.1186/s13058-020-01384-6
Invasive lobular carcinoma of the breast: the increasing importance of this special subtype
Abstract
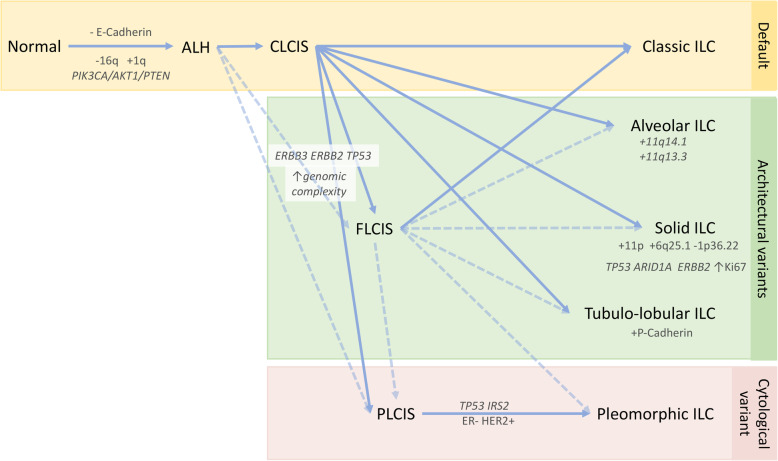
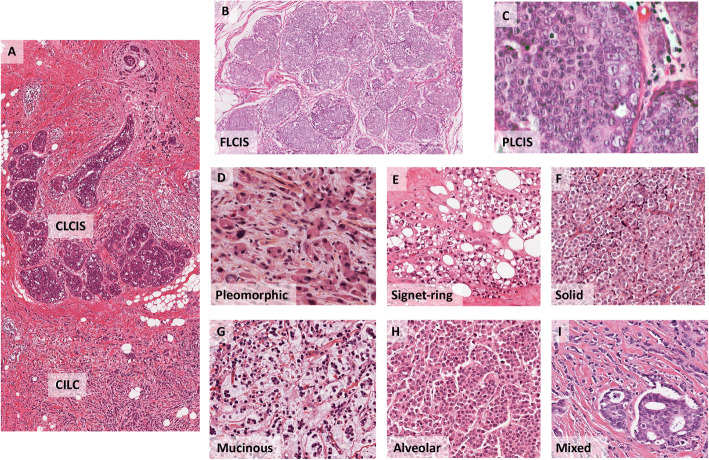
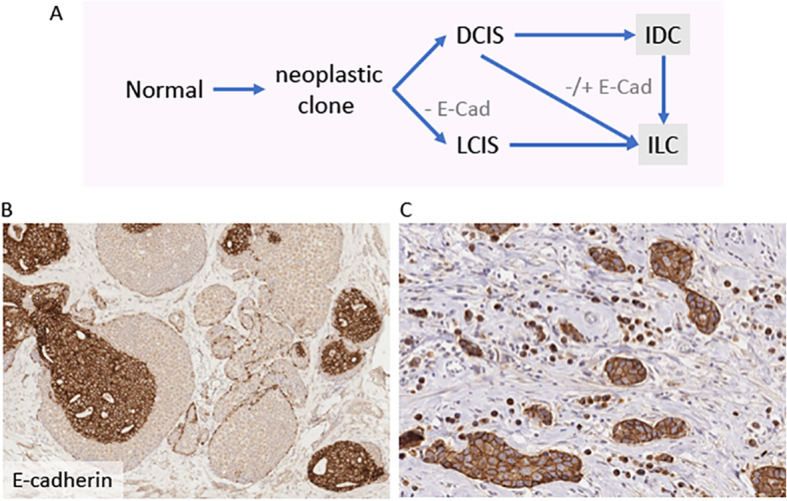
Invasive lobular carcinoma (ILC) is the most common of the breast cancer special types, accounting for up to 15% of all breast cancer cases. ILCs are noted for their lack of E-cadherin function, which underpins their characteristic discohesive growth pattern, with cells arranged in single file and dispersed throughout the stroma. Typically, tumours are luminal in molecular subtype, being oestrogen and progesterone receptor positive, and HER2 negative. Since last reviewing the lobular literature (McCart Reed et al., Breast Cancer Res 17:12, 2015), there has been a considerable increase in research output focused on this tumour type, including studies into the pathology and management of disease, a high-resolution definition of the genomic landscape of tumours as well as the evolution of several potential therapeutic avenues. There abounds a huge amount of new data, which we will review herein.
Keywords: Genomics; ILC; LCIS; Lobular; Lobular breast cancer; Lobular neoplasia; Pathology.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organisation Classification of Tumours Editorial Board. Breast Tumours, 5th edn. Lyon: International Agency for Research on Cancer (IARC); 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
