

Assessment of naive indolent lymphoma using whole-body diffusion-weighted imaging and T2-weighted MRI: results of a prospective study in 30 patients
- PMID: 33413685
- PMCID: PMC7791993
- DOI: 10.1186/s40644-020-00371-6
Assessment of naive indolent lymphoma using whole-body diffusion-weighted imaging and T2-weighted MRI: results of a prospective study in 30 patients
Abstract
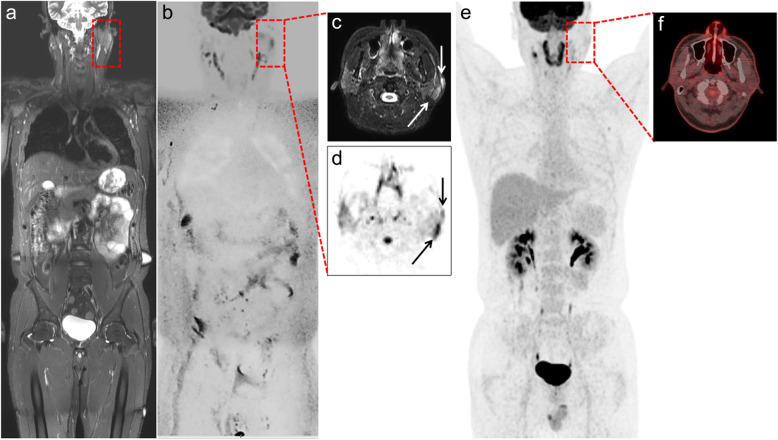
Background: We prospectively evaluated the diagnostic utility of whole-body diffusion-weighted imaging with background body signal suppression and T2-weighted short-tau inversion recovery MRI (WB-DWIBS/STIR) for the pretherapeutic staging of indolent lymphoma in 30 patients.
Methods: This prospective study included 30 treatment-naive patients with indolent lymphomas who underwent WB-DWIBS/STIR and conventional imaging workup plus biopsy. The pretherapeutic staging agreement, sensitivity, and specificity of WB-DWIBS/STIR were investigated with reference to the multimodality and multidisciplinary consensus review for nodal and extranodal lesions excluding bone marrow.
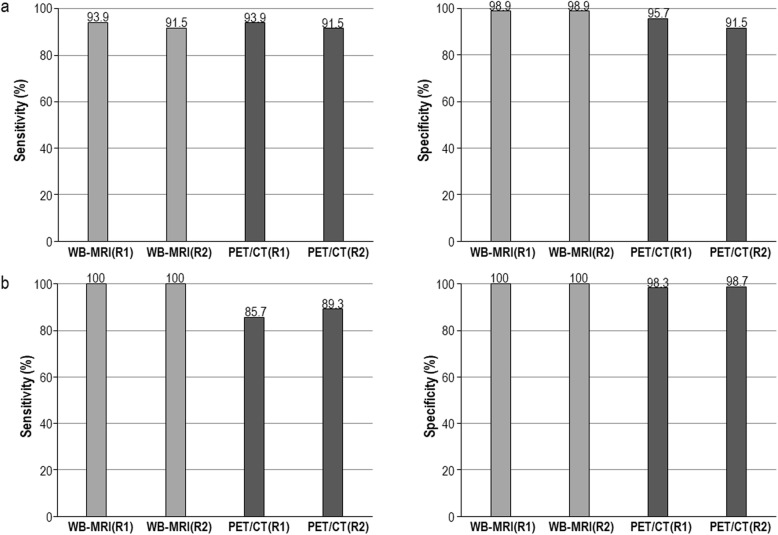
Results: In the pretherapeutic staging, WB-DWIBS/STIR showed very good agreement (κ = 0.96; confidence interval [CI], 0.88-1.00), high sensitivity (93.4-95.1%), and high specificity (99.0-99.4%) for the whole-body regions. These results were similar to those of 18F-FDG-PET/CT, except for the sensitivity for extranodal lesions. For extranodal lesions, WB-DWIBS/STIR showed higher sensitivity compared to 18F-FDG-PET/CT for the whole-body regions (94.9-96.8% vs. 79.6-86.3%, P = 0.058).
Conclusion: WB-DWIBS/STIR is an effective modality for the pretherapeutic staging of indolent lymphoma, and it has benefits when evaluating extranodal lesions, compared with 18F-FDG-PET/CT.
Keywords: Diffusion-weighted imaging with background body signal suppression; Indolent lymphoma; T2-weighted short-tau inversion recovery MRI; Whole-body magnetic resonance imaging.
Conflict of interest statement
The authors declare that they have nothing to disclose.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
