

Correlation of population mortality of COVID-19 and testing coverage: a comparison among 36 OECD countries
- PMID: 33413705
- PMCID: PMC7804083
- DOI: 10.1017/S0950268820003076
Correlation of population mortality of COVID-19 and testing coverage: a comparison among 36 OECD countries
Abstract
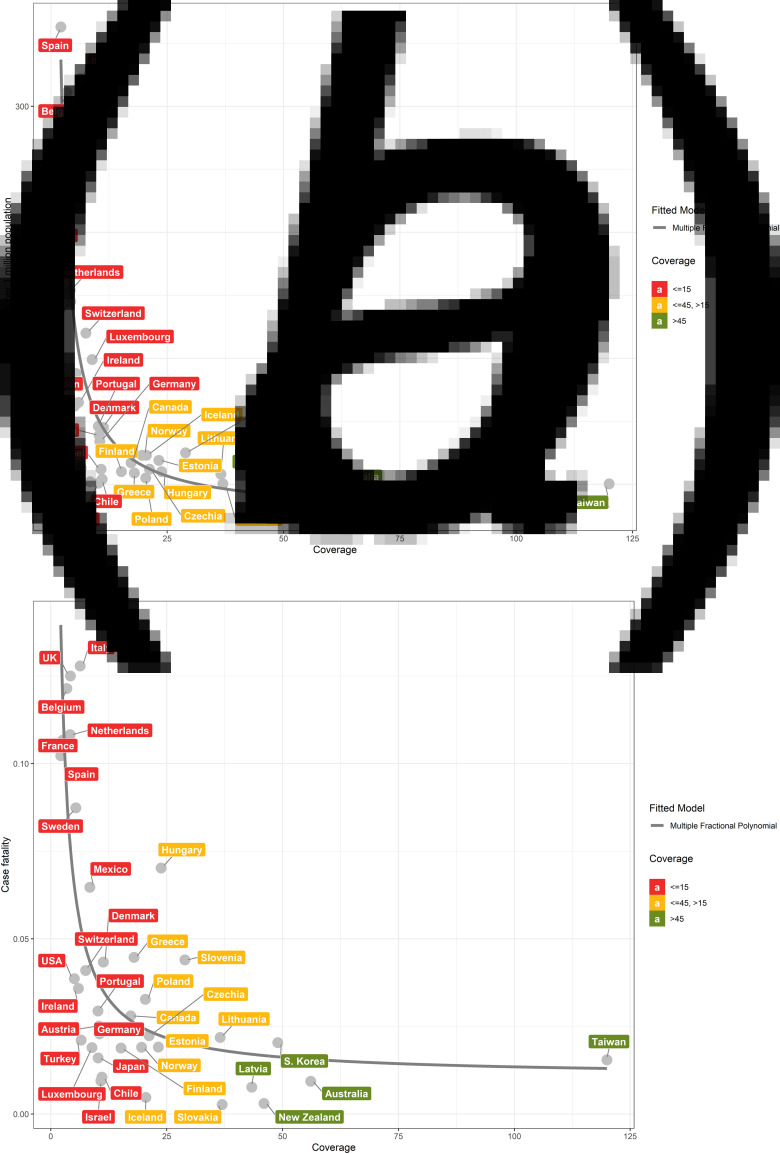
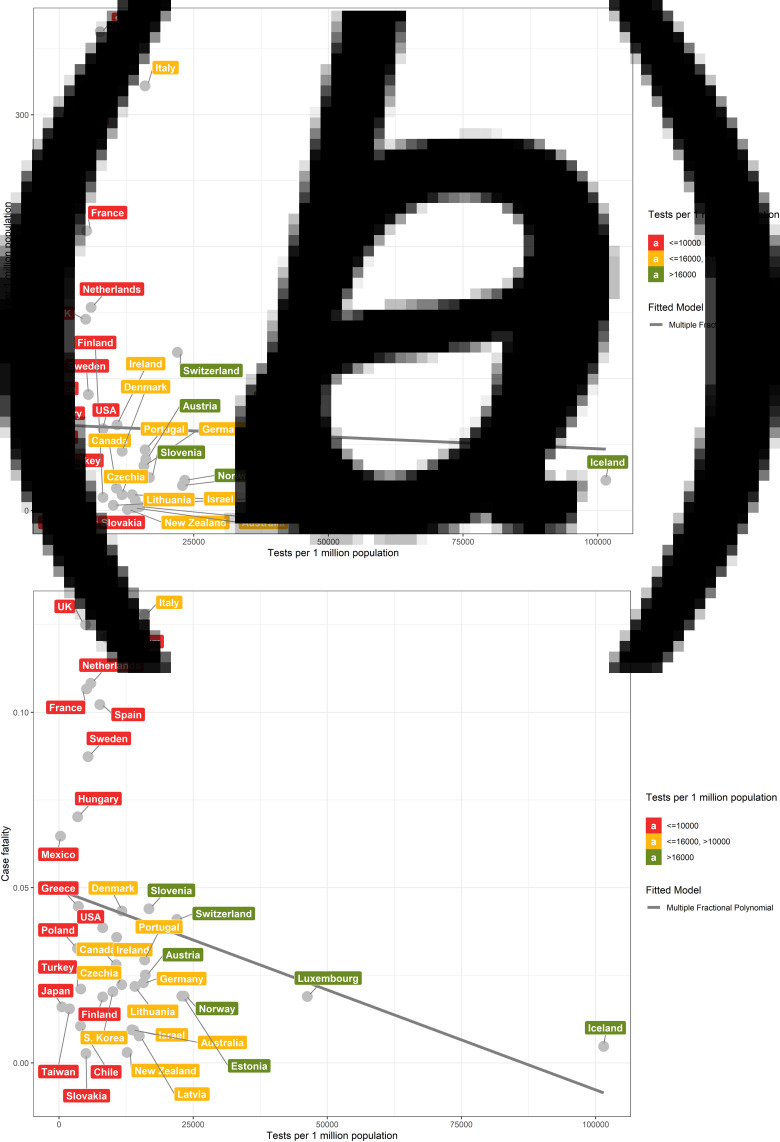
Although testing is widely regarded as critical to fighting the COVID-19 pandemic, what measure and level of testing best reflects successful infection control remains unresolved. Our aim was to compare the sensitivity of two testing metrics - population testing number and testing coverage - to population mortality outcomes and identify a benchmark for testing adequacy. We aggregated publicly available data through 12 April on testing and outcomes related to COVID-19 across 36 OECD (Organization for Economic Development) countries and Taiwan. Spearman correlation coefficients were calculated between the aforementioned metrics and following outcome measures: deaths per 1 million people, case fatality rate and case proportion of critical illness. Fractional polynomials were used to generate scatter plots to model the relationship between the testing metrics and outcomes. We found that testing coverage, but not population testing number, was highly correlated with population mortality (rs = -0.79, P = 5.975 × 10-9vs. rs = -0.3, P = 0.05) and case fatality rate (rs = -0.67, P = 9.067 × 10-6vs. rs = -0.21, P = 0.20). A testing coverage threshold of 15-45 signified adequate testing: below 15, testing coverage was associated with exponentially increasing population mortality; above 45, increased testing did not yield significant incremental mortality benefit. Taken together, testing coverage was better than population testing number in explaining country performance and can serve as an early and sensitive indicator of testing adequacy and disease burden.
Keywords: COVID-19; SARS-CoV-2; testing coverage.
Conflict of interest statement
The authors disclose no conflicts of interest.
Figures
References
-
- COVID-19 Map. Johns Hopkins Coronavirus Resource Center. Available at https://coronavirus.jhu.edu/map.html (Accessed 14 May 2020).
-
- Correcting under-reported COVID-19 case numbers: estimating the true scale of the pandemic|medRxiv. Available at https://www.medrxiv.org/content/10.1101/2020.03.14.20036178v2 (Accessed 24 April 2020).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
