

Molecular Characterization and Therapeutic Targeting of Colorectal Cancers Harboring Receptor Tyrosine Kinase Fusions
- PMID: 33414136
- PMCID: PMC9063924
- DOI: 10.1158/1078-0432.CCR-20-4073
Molecular Characterization and Therapeutic Targeting of Colorectal Cancers Harboring Receptor Tyrosine Kinase Fusions
Abstract
Purpose: Receptor tyrosine kinase fusions in colorectal cancers are rare, but potentially therapeutically relevant. We describe clinical, molecular, and pathologic attributes of RTK fusion-associated colorectal cancer.
Experimental design: We identified all cases with RTK fusions in patients with colorectal cancer seen at Dana-Farber Cancer Institute (Boston, MA) who underwent OncoPanel testing between 2013 and 2018. Clinical, histologic, and molecular features were extracted from the patient charts and molecular testing results.
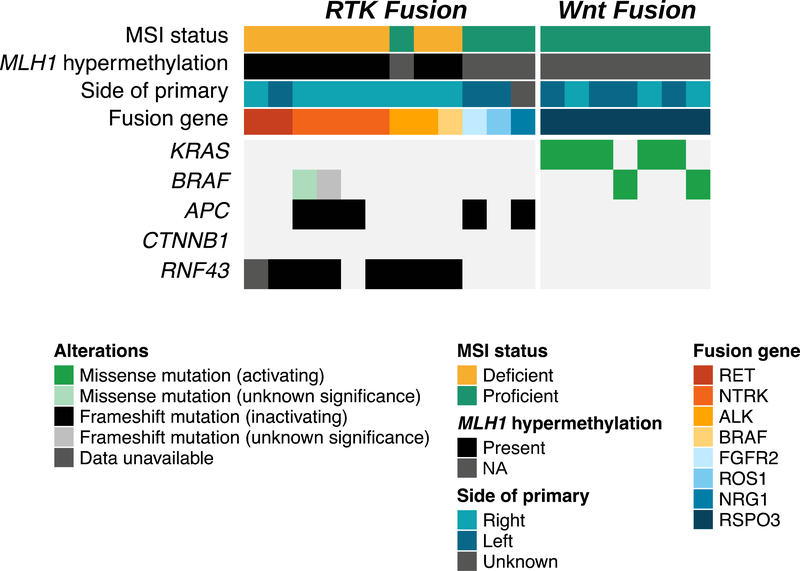
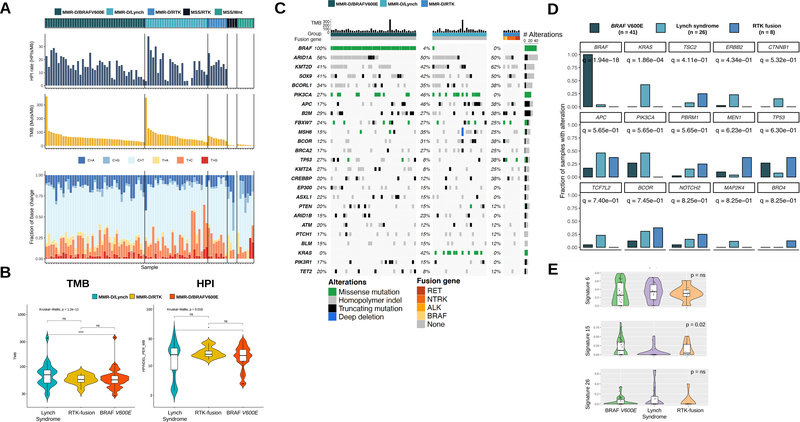
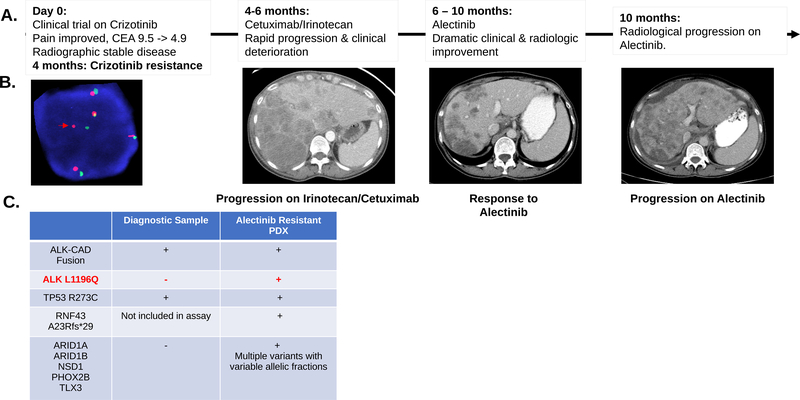
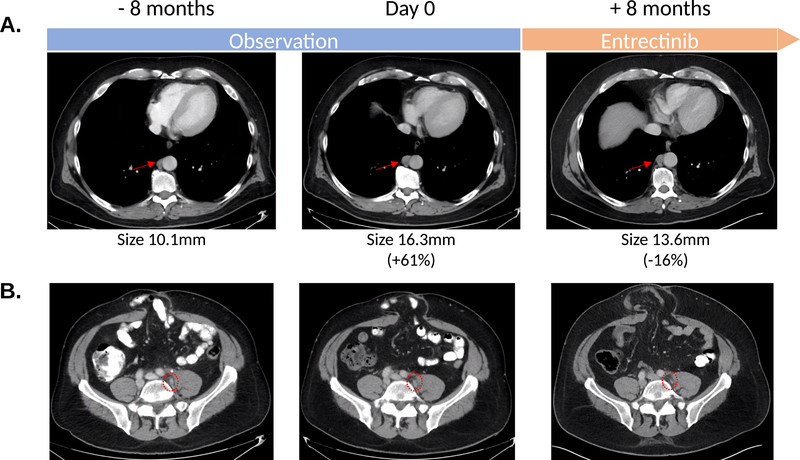
Results: We identified 12 driver oncogenic fusions in various RTKs. These fusions occurred exclusively in BRAF and RAS wild-type tumors and were enriched in right-sided and mismatch repair-deficient (MMR-D) colorectal cancers. All of the MMR-D colorectal cancers with RTK fusions were found in tumors with acquired MMR-D due to MLH1 promoter hypermethylation and one was associated with a sessile serrated polyp. Molecular profiles of MMR-D colorectal cancer with RTK fusions largely resembled BRAF V600E-mutated MMR-D colorectal cancer, rather than those secondary to Lynch syndrome. We describe two patients with fusion-associated microsatellite stable (MSS) colorectal cancer who derived clinical benefit from therapeutic targeting of their translocation. The first harbored an ALK-CAD fusion and received sequential crizotinib and alectinib therapy for a total of 7.5 months until developing an ALK L1196Q gatekeeper mutation. The second patient, whose tumor contained an ROS1-GOPC fusion, continues to benefit from entrectinib after 9 months of therapy.
Conclusions: RTK fusions in colorectal cancer are a rare, but important disease subgroup that occurs in RAS and BRAF wild-type tumors. Despite enrichment in acquired MMR-D tumors, RTK fusions also occur in MSS colorectal cancer and provide an important therapeutic target.
©2021 American Association for Cancer Research.
Figures
References
-
- Sartore-Bianchi A, Trusolino L, Martino C, Bencardino K, Lonardi S, Bergamo F, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol 2016;17(6):738–46 doi 10.1016/S1470-2045(16)00150-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
