

Mass Disasters and Burnout in Nephrology Personnel: From Earthquakes and Hurricanes to COVID-19 Pandemic
- PMID: 33414153
- PMCID: PMC8259469
- DOI: 10.2215/CJN.08400520
Mass Disasters and Burnout in Nephrology Personnel: From Earthquakes and Hurricanes to COVID-19 Pandemic
Abstract
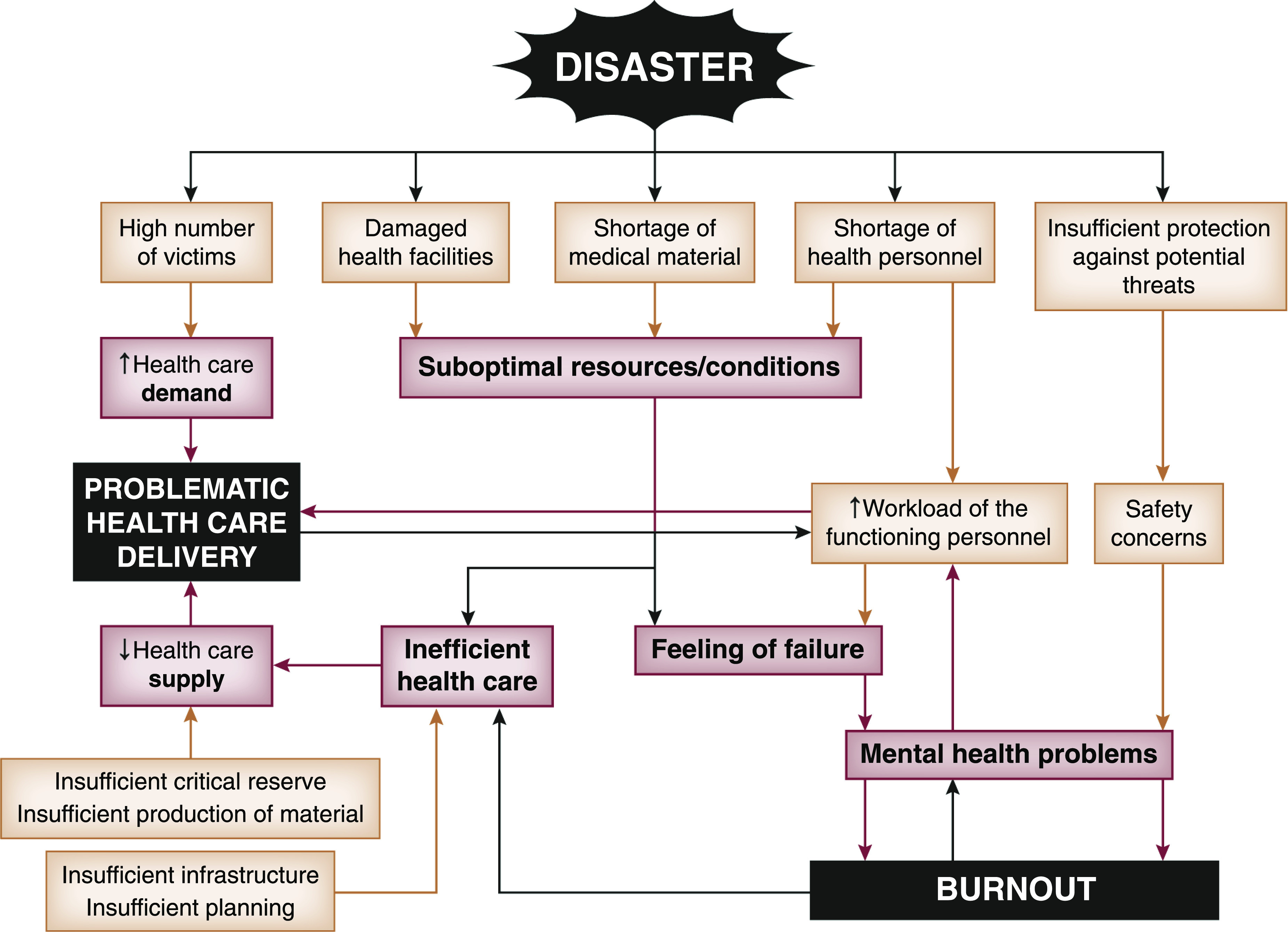
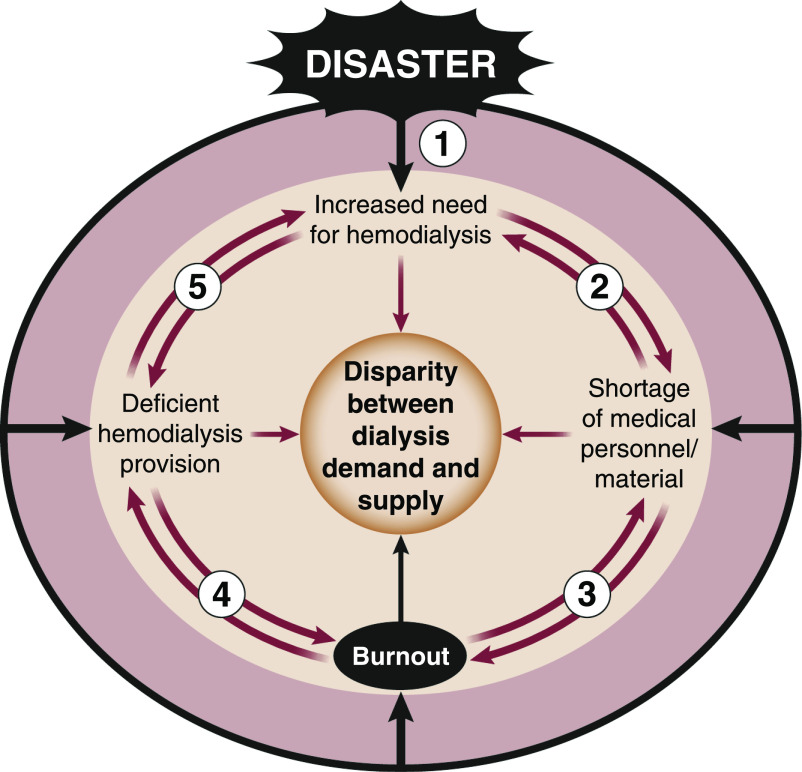
Mass disasters result in extensive health problems and make health care delivery problematic, as has been the case during the COVID-19 pandemic. Although COVID-19 was initially considered a pulmonary problem, it soon became clear that various other organs were involved. Thus, many care providers, including kidney health personnel, were overwhelmed or developed burnout. This review aims to describe the spectrum of burnout in mass disasters and suggests solutions specifically for nephrology personnel by extending previous experience to the COVID-19 pandemic. Burnout (a psychologic response to work-related stress) is already a frequent part of routine nephrology practice and, not surprisingly, is even more common during mass disasters due to increased workload and specific conditions, in addition to individual factors. Avoiding burnout is essential to prevent psychologic and somatic health problems in personnel as well as malpractice, understaffing, and inadequate health care delivery, all of which increase the health care burden of disasters. Burnout may be prevented by predisaster organizational measures, which include developing an overarching plan and optimizing health care infrastructure, and ad hoc disaster-specific measures that encompass both organizational and individual measures. Organizational measures include increasing safety, decreasing workload and fear of malpractice, optimizing medical staffing and material supplies, motivating personnel, providing mental health support, and enabling flexibility in working circumstances. Individual measures include training on coping with stress and problematic conditions, minimizing the stigma of emotional distress, and maintaining physical health. If these measures fall short, asking for external help is mandatory to avoid an inefficient disaster health care response. Minimizing burnout by applying these measures will improve health care provision, thus saving as many lives as possible.
Keywords: COVID-19; burnout; earthquake; hurricane; massive disaster; nephrology; pandemic.
Copyright © 2021 by the American Society of Nephrology.
Figures
Similar articles
-
Burnout among healthcare providers during COVID-19: Challenges and evidence-based interventions.Indian J Med Ethics. 2020 Oct-Dec;V(4):1-6. doi: 10.20529/IJME.2020.73. Indian J Med Ethics. 2020. PMID: 34018959
-
[Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks?].Encephale. 2020 Jun;46(3S):S73-S80. doi: 10.1016/j.encep.2020.04.008. Epub 2020 Apr 22. Encephale. 2020. PMID: 32370984 Free PMC article. French.
-
Maladaptive behaviors in disasters: case study evaluation of Hurricane Hugo, Hurricane Katrina and the Haiti Earthquake.Front Public Health. 2024 Aug 27;12:1396517. doi: 10.3389/fpubh.2024.1396517. eCollection 2024. Front Public Health. 2024. PMID: 39257945 Free PMC article. Review.
-
Natural disasters and dialysis care in the Asia-Pacific.Nephrology (Carlton). 2015 Dec;20(12):873-80. doi: 10.1111/nep.12522. Nephrology (Carlton). 2015. PMID: 26032113 Review.
-
Conflict Nephrology: War and Natural Disasters.Kidney360. 2023 Mar 1;4(3):405-408. doi: 10.34067/KID.0000000000000071. Kidney360. 2023. PMID: 36763799 Free PMC article.
Cited by
-
Destructive disasters, trauma, crush syndrome, and beyond.Acta Orthop Traumatol Turc. 2023 Nov;57(6):305-314. doi: 10.5152/j.aott.2023.23147. Acta Orthop Traumatol Turc. 2023. PMID: 38454211 Free PMC article.
-
Mortality associated with the COVID-19 pandemic in the Swiss dialysis population beyond SARS-CoV-2 infection.Clin Kidney J. 2024 Oct 29;17(12):sfae322. doi: 10.1093/ckj/sfae322. eCollection 2024 Dec. Clin Kidney J. 2024. PMID: 39664996 Free PMC article.
-
Disaster preparedness and kidney health in children.Pediatr Nephrol. 2025 Jul;40(7):2133-2143. doi: 10.1007/s00467-025-06693-6. Epub 2025 Feb 4. Pediatr Nephrol. 2025. PMID: 39903241 Review.
-
The Global Impact of the COVID-19 Pandemic on In-Center Hemodialysis Services: An ISN-Dialysis Outcomes Practice Patterns Study Survey.Kidney Int Rep. 2022 Mar;7(3):397-409. doi: 10.1016/j.ekir.2021.12.011. Epub 2021 Dec 13. Kidney Int Rep. 2022. PMID: 34957349 Free PMC article.
-
Changes of Acute Kidney Injury Epidemiology during the COVID-19 Pandemic: A Retrospective Cohort Study.J Clin Med. 2022 Jun 10;11(12):3349. doi: 10.3390/jcm11123349. J Clin Med. 2022. PMID: 35743418 Free PMC article.
References
-
- World Health Organization (WHO) : Glossary of humanitarian terms. Available at: https://www.who.int/hac/about/reliefweb-aug2008.pdf. Accessed November 6, 2020
-
- Guha-Sapir D, Hoyois P; EM-DAT: The International Disaster database, general classification of disasters. Available at: https://www.emdat.be/classification/. Accessed November 6, 2020
-
- Sever MS, Vanholder R; RDRTF of ISN Work Group on Recommendations for the Management of Crush Victims in Mass Disasters: Recommendation for the management of crush victims in mass disasters. Nephrol Dial Transplant 27[Suppl 1]: i1–i67, 2012. - PubMed
-
- World Health Organization : Coronavirus disease (COVID-2019) situation reports. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed November 6, 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
