

Dural Venous Sinus Stenosis: Why Distinguishing Intrinsic-versus-Extrinsic Stenosis Matters
- PMID: 33414231
- PMCID: PMC7872181
- DOI: 10.3174/ajnr.A6890
Dural Venous Sinus Stenosis: Why Distinguishing Intrinsic-versus-Extrinsic Stenosis Matters
Abstract
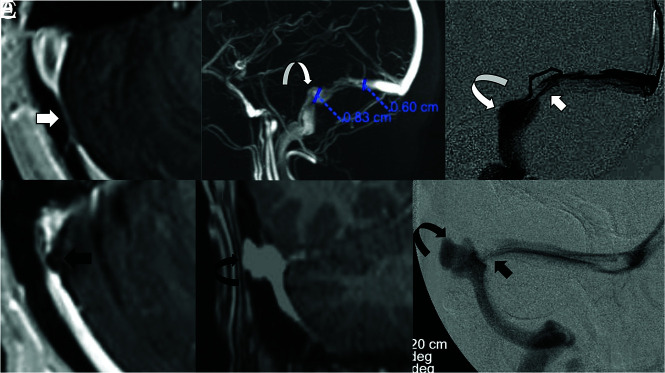
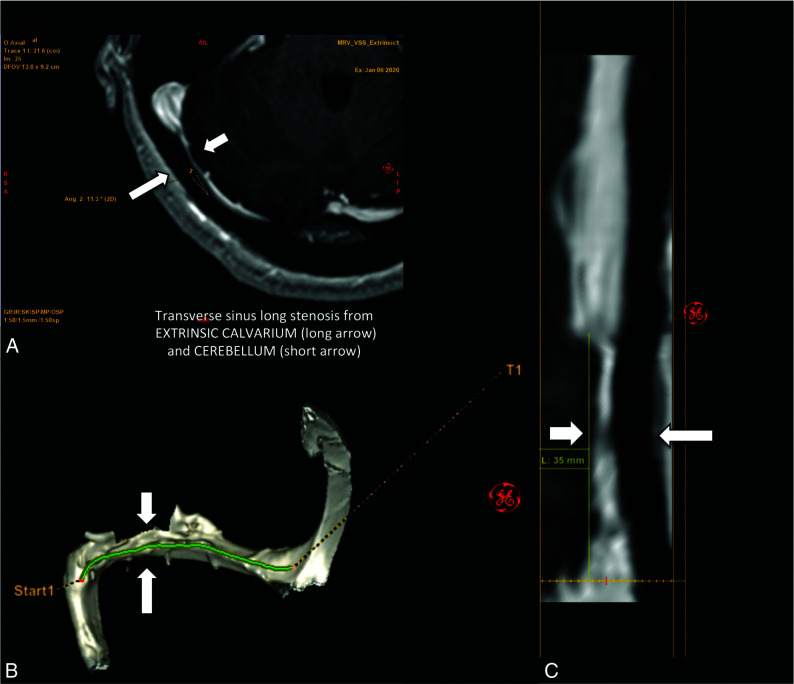
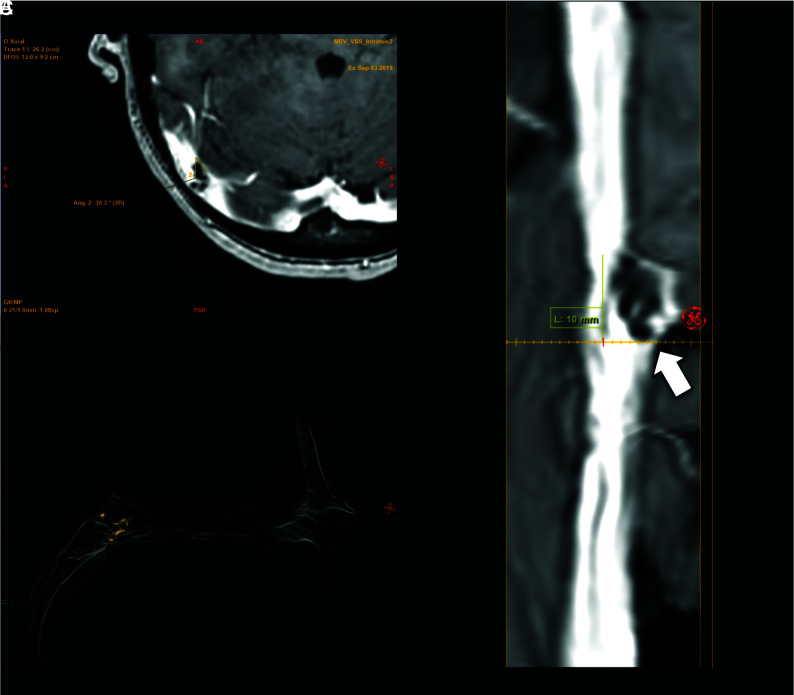
Background and purpose: Dural venous sinus stenosis has been associated with idiopathic intracranial hypertension and isolated venous pulsatile tinnitus. However, the utility of characterizing stenosis as intrinsic or extrinsic remains indeterminate. The aim of this retrospective study was to review preprocedural imaging of patients with symptomatic idiopathic intracranial hypertension and pulsatile tinnitus, classify the stenosis, and assess a trend between stenosis type and clinical presentation while reviewing the frequencies of other frequently seen imaging findings in these conditions.
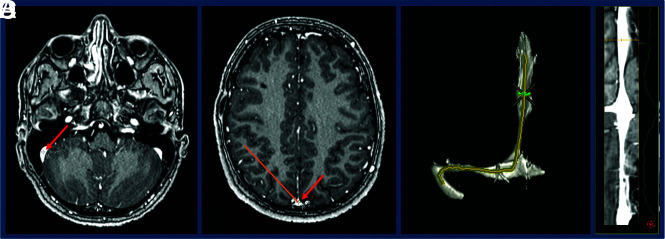
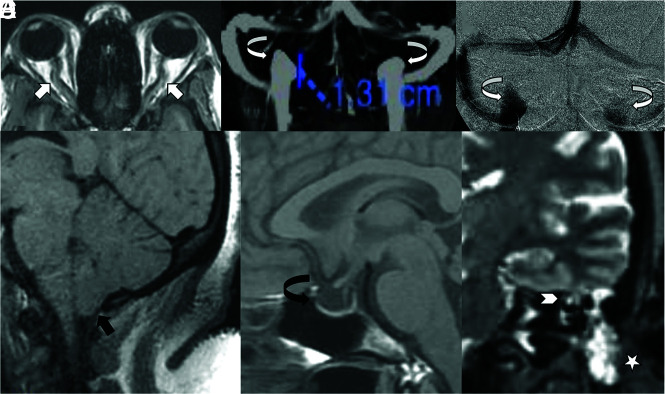
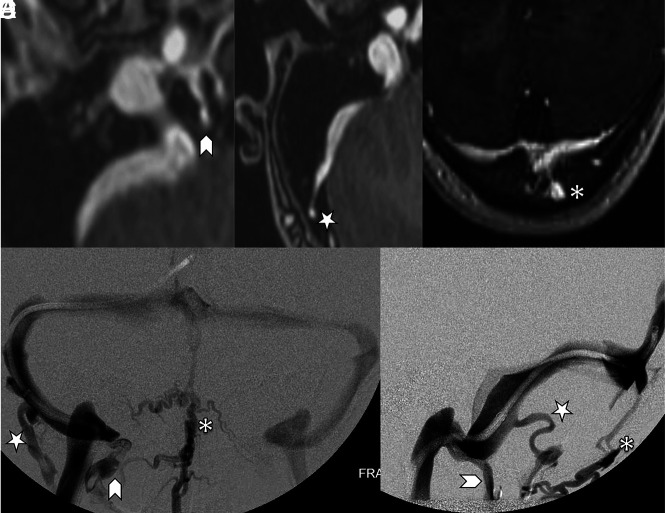
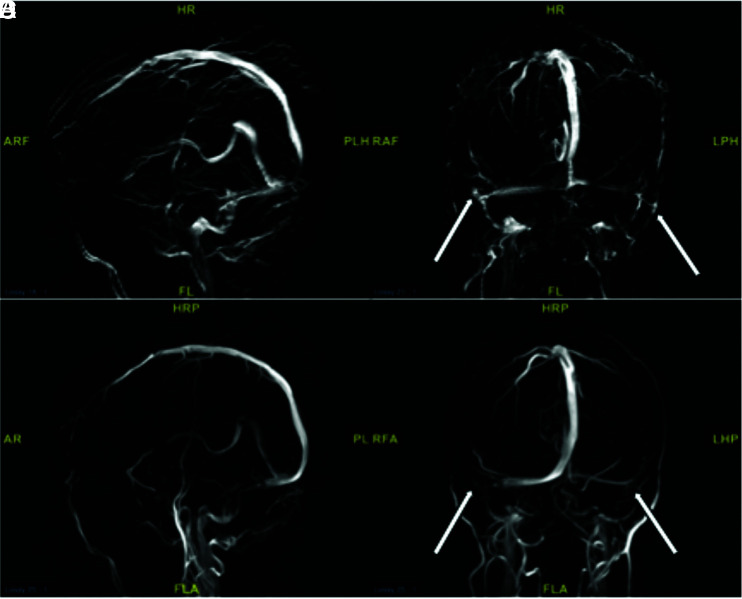
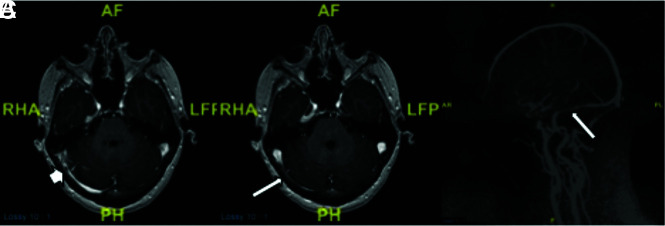
Materials and methods: MRVs of 115 patients with idiopathic intracranial hypertension and 43 patients with pulsatile tinnitus before venous sinus stent placement were reviewed. Parameters recorded included the following: intrinsic or extrinsic stenosis, prominent emissary veins, optic nerve tortuosity, cephalocele, sella appearance, poststenotic fusiform enlargement versus saccular venous aneurysm, and internal jugular bulb diverticula. χ2 cross-tabulation statistics were calculated and recorded for all data.
Results: Most patients with idiopathic intracranial hypertension (75 of 115 sinuses, 65%) had extrinsic stenosis, and most patients with pulsatile tinnitus (37 of 45 sinuses, 82%) had intrinsic stenosis. Marked optic nerve tortuosity was more common in idiopathic intracranial hypertension. Cephaloceles were rare in both cohorts, with an increased trend toward the presence in idiopathic intracranial hypertension. Empty sellas were more common in idiopathic intracranial hypertension. Cerebellar tonsils were similarly located at the foramen magnum level in both cohorts. Saccular venous aneurysms were more common in pulsatile tinnitus. Internal jugular bulb diverticula were similarly common in both cohorts.
Conclusions: In this cohort, most patients with idiopathic intracranial hypertension had extrinsic stenosis, and most patients with pulsatile tinnitus had intrinsic stenosis. Awareness and reporting of these subtypes may reduce the underrecognition of potential contributory stenoses in a given patient's idiopathic intracranial hypertension or pulsatile tinnitus.
© 2021 by American Journal of Neuroradiology.
Figures
Comment in
-
Cerebral Venous Wall Diseases: The Other Side of the Picture.AJNR Am J Neuroradiol. 2021 Jan;42(2):297-298. doi: 10.3174/ajnr.A6914. Epub 2021 Jan 7. AJNR Am J Neuroradiol. 2021. PMID: 33414232 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical