

Timing of Co-occurring Chronic Conditions in Children With Neurologic Impairment
- PMID: 33414236
- PMCID: PMC7849195
- DOI: 10.1542/peds.2020-009217
Timing of Co-occurring Chronic Conditions in Children With Neurologic Impairment
Abstract
Background: Children with neurologic impairment (NI) are at risk for developing co-occurring chronic conditions, increasing their medical complexity and morbidity. We assessed the prevalence and timing of onset for those conditions in children with NI.
Methods: This longitudinal analysis included 6229 children born in 2009 and continuously enrolled in Medicaid through 2015 with a diagnosis of NI by age 3 in the IBM Watson Medicaid MarketScan Database. NI was defined with an existing diagnostic code set encompassing neurologic, genetic, and metabolic conditions that result in substantial functional impairments requiring subspecialty medical care. The prevalence and timing of co-occurring chronic conditions was assessed with the Agency for Healthcare Research and Quality Chronic Condition Indicator system. Mean cumulative function was used to measure age trends in multimorbidity.
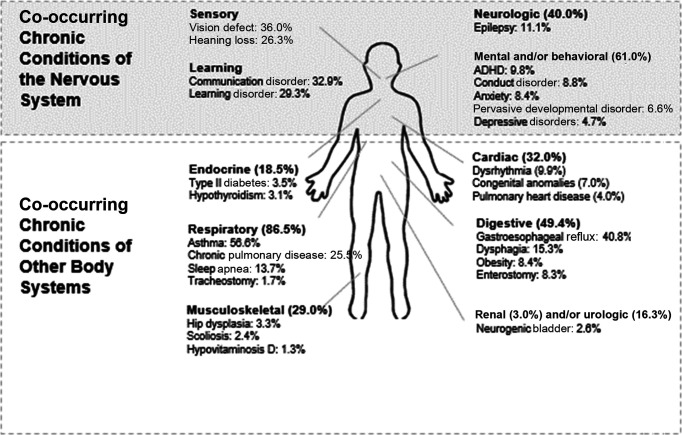
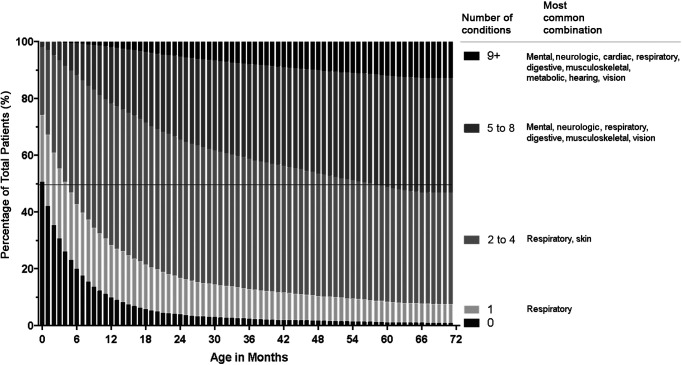
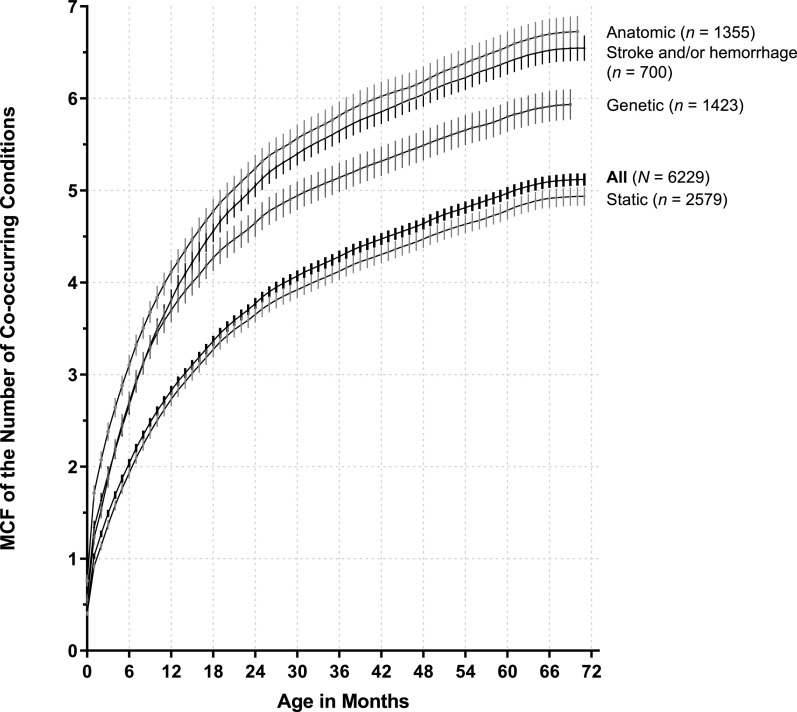
Results: The most common type of NI was static (56.3%), with cerebral palsy (10.0%) being the most common NI diagnosis. Respiratory (86.5%) and digestive (49.4%) organ systems were most frequently affected by co-occurring chronic conditions. By ages 2, 4, and 6 years, the mean (95% confidence interval [CI]) numbers of co-occurring chronic conditions were 3.7 (95% CI 3.7-3.8), 4.6 (95% CI 4.5-4.7), and 5.1 (95% CI 5.1-5.2). An increasing percentage of children had ≥9 co-occurring chronic conditions as they aged: 5.3% by 2 years, 10.0% by 4 years, and 12.8% by 6 years.
Conclusions: Children with NI enrolled in Medicaid have substantial multimorbidity that develops early in life. Increased attention to the timing and types of multimorbidity in children with NI may help optimize their preventive care and case management health services.
Copyright © 2021 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Venkateswaran S, Shevell MI. Comorbidities and clinical determinants of outcome in children with spastic quadriplegic cerebral palsy. Dev Med Child Neurol. 2008;50(3):216–222 - PubMed
-
- Strauss D, Brooks J, Rosenbloom L, Shavelle R. Life expectancy in cerebral palsy: an update. Dev Med Child Neurol. 2008;50(7):487–493 - PubMed
-
- Strauss D, Shavelle R, Reynolds R, Rosenbloom L, Day S. Survival in cerebral palsy in the last 20 years: signs of improvement? Dev Med Child Neurol. 2007;49(2):86–92 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
