

Retrospective analysis of the Italian exit strategy from COVID-19 lockdown
- PMID: 33414277
- PMCID: PMC7848712
- DOI: 10.1073/pnas.2019617118
Retrospective analysis of the Italian exit strategy from COVID-19 lockdown
Abstract
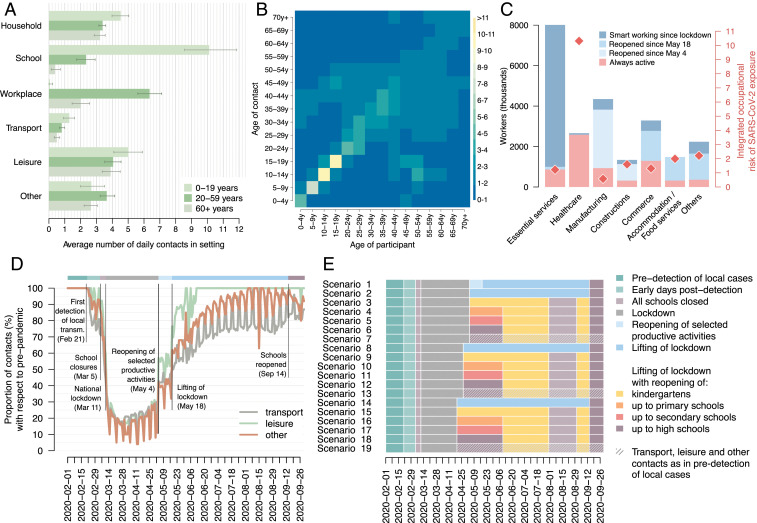
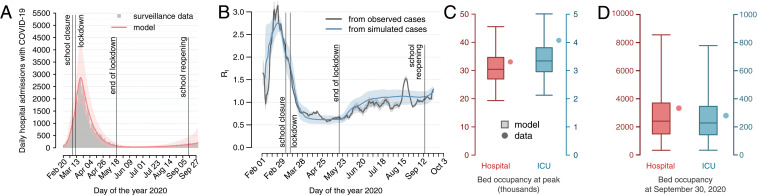
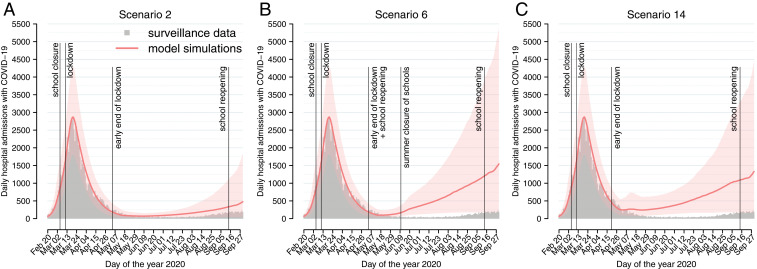
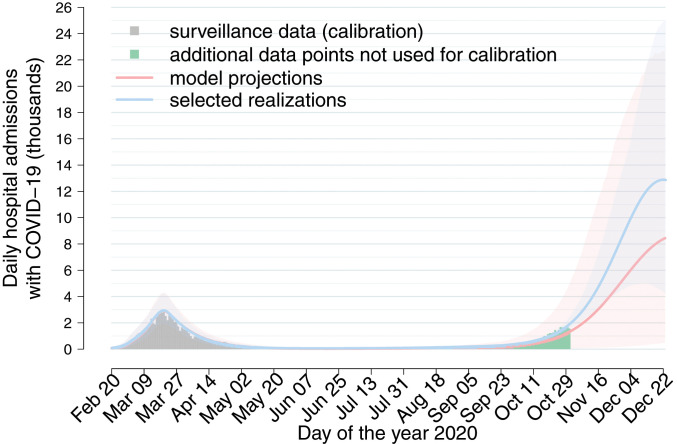
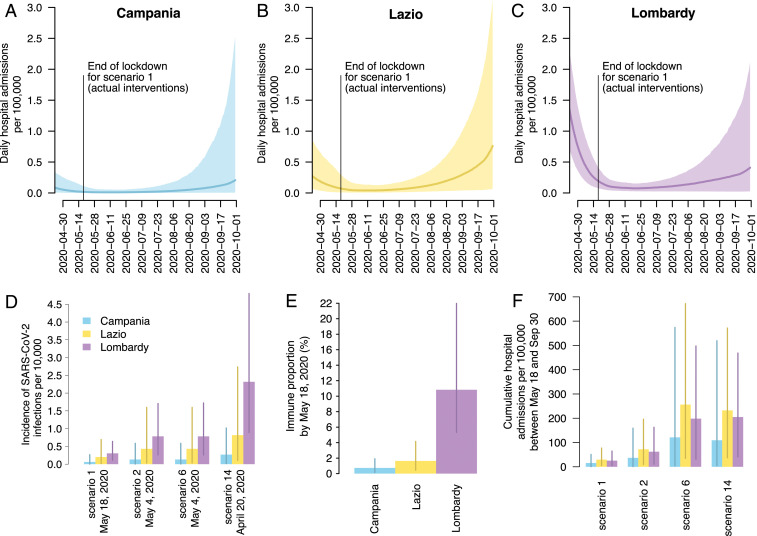
After the national lockdown imposed on March 11, 2020, the Italian government has gradually resumed the suspended economic and social activities since May 4, while maintaining the closure of schools until September 14. We use a model of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission to estimate the health impact of different exit strategies. The strategy adopted in Italy kept the reproduction number Rt at values close to one until the end of September, with marginal regional differences. Based on the estimated postlockdown transmissibility, reopening of workplaces in selected industrial activities might have had a minor impact on the transmissibility. Reopening educational levels in May up to secondary schools might have influenced SARS-CoV-2 transmissibility only marginally; however, including high schools might have resulted in a marked increase of the disease burden. Earlier reopening would have resulted in disproportionately higher hospitalization incidence. Given community contacts in September, we project a large second wave associated with school reopening in the fall.
Keywords: SARS-CoV-2; mathematical modeling; reopening scenarios.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: M.A. has received research funding from Seqirus. The funding is not related to COVID-19. All other authors declare no competing interest.
Figures
References
-
- World Health Organization , WHO Director-General’s opening remarks at the media briefing on COVID-19. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re.... Accessed 1 December 2020.
-
- International Monetary Fund , Policy responses to COVID-19. https://www.imf.org/en/Topics/imf-and-covid19/Policy-Responses-to-COVID-19. Accessed 1 December 2020.
-
- Decree of the Prime Minister , Ulteriori disposizioni attuative del decreto-legge 23 febbraio 2020, n. 6, recante misure urgenti in materia di contenimento e gestione dell’emergenza epidemiologica da COVID-19, applicabili sull’intero territorio nazionale. https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73643. Accessed 1 December 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
