

Effect of autologous hematopoietic stem cell transplant on the development of second primary malignancies in multiple myeloma patients
- PMID: 33414400
- PMCID: PMC7791054
- DOI: 10.1038/s41408-020-00400-4
Effect of autologous hematopoietic stem cell transplant on the development of second primary malignancies in multiple myeloma patients
Abstract
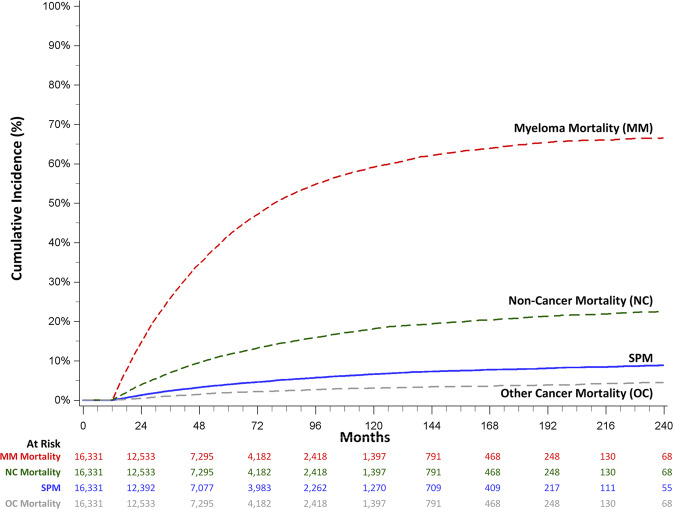
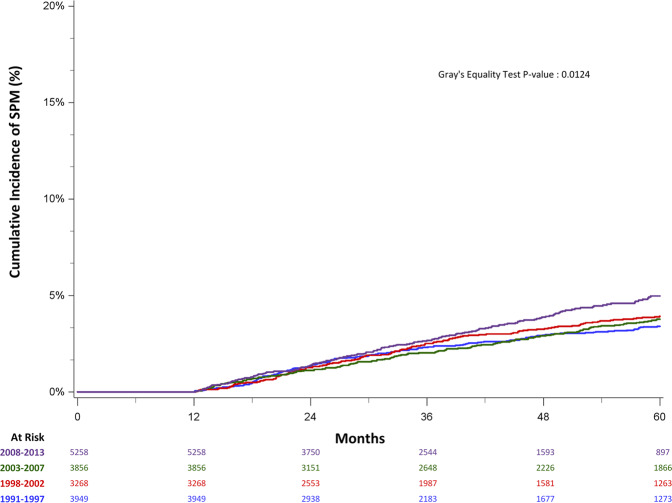
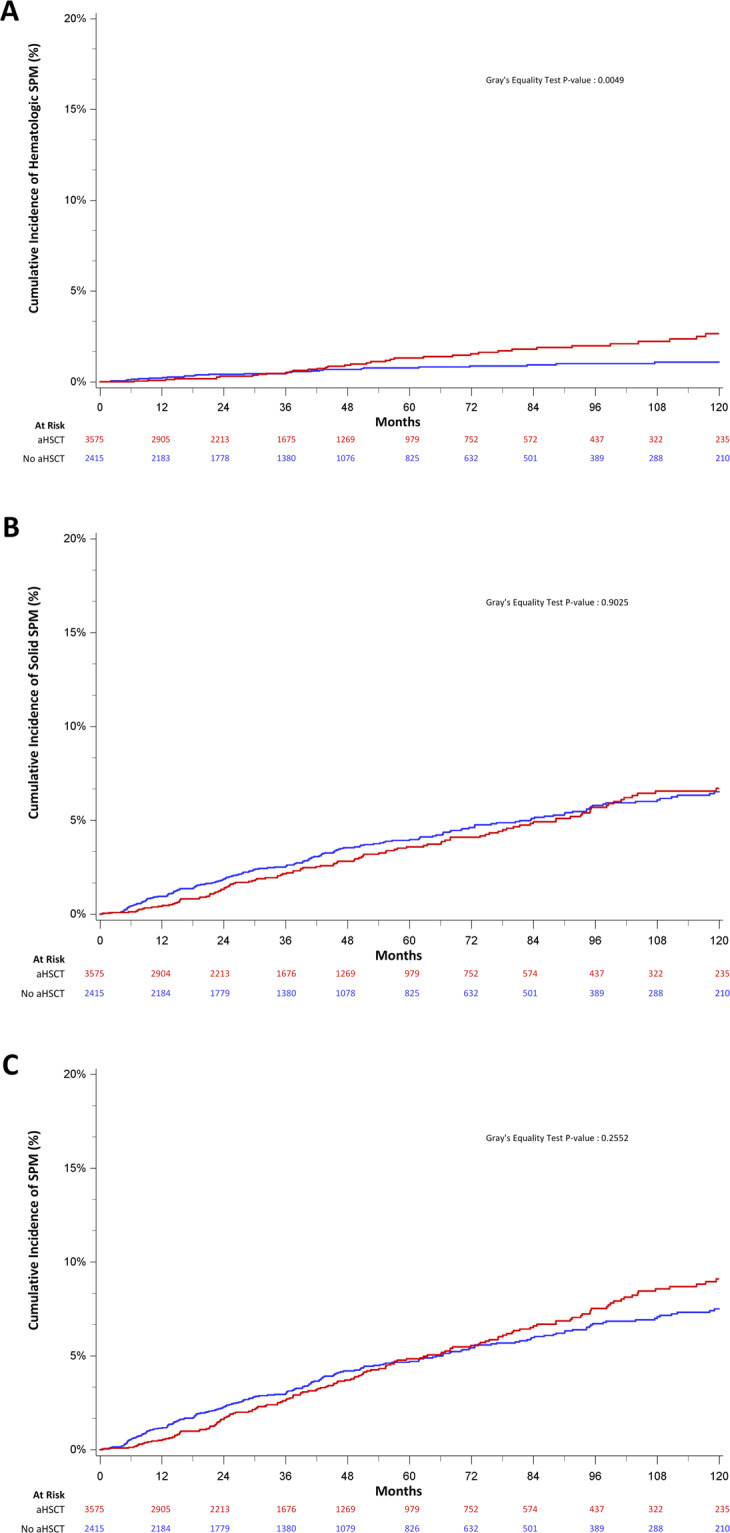
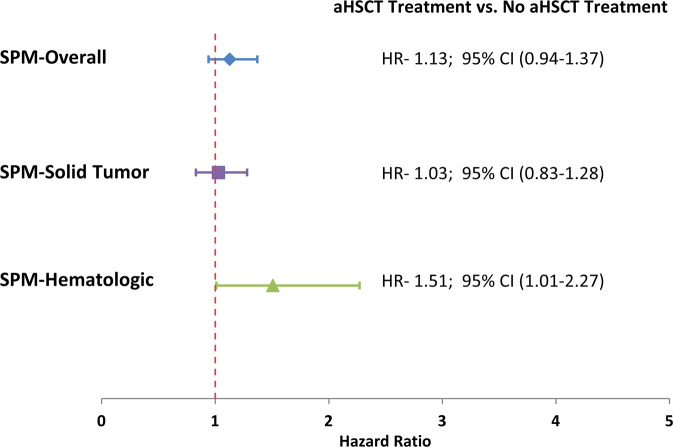
Autologous stem cell transplant (aHSCT) is associated with improved survival for multiple myeloma (MM) patients but may be associated with second primary malignancy (SPM) development. Using the California Cancer Registry linked to statewide hospitalization data, we determined the cumulative incidence (CMI) of SPMs more than 1 year after MM diagnosis, accounting for the competing risk of death. AHSCT recipients were matched 1:2 to non-aHSCT patients. Adjusted hazard ratios (aHR) were estimated using the Fine and Gray method. Among 16,331 patients, 933 (5.7%) developed a SPM more than 1 year after diagnosis. The 10-year CMI of developing any SPM was 6.6%, 5.7% for solid tumor SPM and 0.9% for hematologic malignancies. The 10-year CMI of developing any SPM was similar among aHSCT [9.1% (7.7-10.7%)] and non-aHSCT [7.5% (6.5-8.6%)] (P = 0.26) recipients and there was no difference in solid-tumor SPMs (P = 0.98). The 10-year CMI of hematologic SPMs was higher among aHSCT recipients [2.1% (1.4-2.9%) vs. 0.8% (0.5-1.2%); P = 0.005], corresponding to a 1.3% absolute increase and an aHR of 1.51 (1.01-2.27). Ten-year myeloma-specific and non-cancer mortality rates were 59% (58.2-60.0%) and 18.1% (17.4-18.8%), respectively. Although aHSCT was associated with a small increase in hematologic SPMs, mortality was driven by MM and non-cancer causes.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
