

Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase: ENESTnd 10-year analysis
- PMID: 33414482
- PMCID: PMC7862065
- DOI: 10.1038/s41375-020-01111-2
Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase: ENESTnd 10-year analysis
Erratum in
-
Correction to: Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase: ENESTnd 10-year analysis.Leukemia. 2021 Jul;35(7):2142-2143. doi: 10.1038/s41375-021-01306-1. Leukemia. 2021. PMID: 34108614 Free PMC article. No abstract available.
Abstract
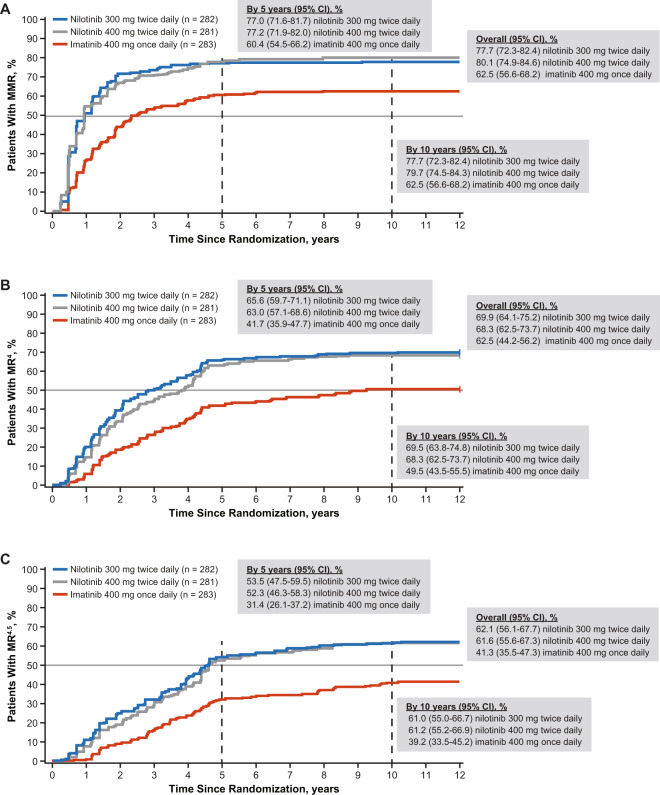
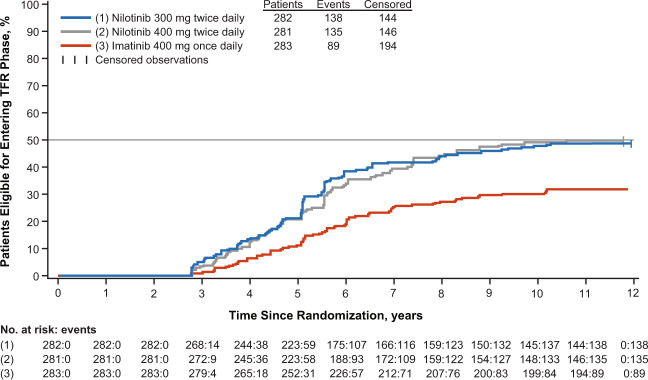
In the ENESTnd study, with ≥10 years follow-up in patients with newly diagnosed chronic myeloid leukemia (CML) in chronic phase, nilotinib demonstrated higher cumulative molecular response rates, lower rates of disease progression and CML-related death, and increased eligibility for treatment-free remission (TFR). Cumulative 10-year rates of MMR and MR4.5 were higher with nilotinib (300 mg twice daily [BID], 77.7% and 61.0%, respectively; 400 mg BID, 79.7% and 61.2%, respectively) than with imatinib (400 mg once daily [QD], 62.5% and 39.2%, respectively). Cumulative rates of TFR eligibility at 10 years were higher with nilotinib (300 mg BID, 48.6%; 400 mg BID, 47.3%) vs imatinib (29.7%). Estimated 10-year overall survival rates in nilotinib and imatinib arms were 87.6%, 90.3%, and 88.3%, respectively. Overall frequency of adverse events was similar with nilotinib and imatinib. By 10 years, higher cumulative rates of cardiovascular events were reported with nilotinib (300 mg BID, 16.5%; 400 mg BID, 23.5%) vs imatinib (3.6%), including in Framingham low-risk patients. Overall efficacy and safety results support the use of nilotinib 300 mg BID as frontline therapy for optimal long-term outcomes, especially in patients aiming for TFR. The benefit-risk profile in context of individual treatment goals should be carefully assessed.
Conflict of interest statement
HMK, Grants, honoraria: AbbVie, Agios, Amgen, Immunogen, Pfizer. Grants: Ariad, Astex, BMS, Cyclacel, Daiichi Sankyo, Jazz Pharmaceuticals, Novartis. Advisory boards: Actinium. Consulting: Novartis. Honoraria: Takeda. TPH, Grants, advisory boards, symposia: Novartis. Grants: BMS. RAL, Personal fees, clinical trials contracts: Novartis. D-WK, Grants: Novartis, BMS, Pfizer, ILYANG co. SI, none. PlC, Speaker, honoraria: Novartis, BMS, Pfizer, Incyte. GE, Personal fees, nonfinancial support: Novartis. Personal fees: BMS, Pfizer, Incyte. CB, Personal fees, speaker, advisory boards: Novartis. Personal fees, speaker: EMS. RP, none. REC, Grants, personal fees: Novartis. Grants, personal fees: BMS, Pfizer. Personal fees: Ariad/Incyte. VD, none. IWF, Grants, other funding: AbbVie, AstraZeneca, BeiGene, Gilead Sciences, Janssen, Juno Therapeutics, Kite Pharma, MorphoSys, Pharmacyclics, Roche, Seattle Genetics, Takeda, TG Therapeutics, Unum Therapeutics, Verastem. Other funding: Curio Science, Great Point Partners, Iksuda Therapeutics, Nurix Therapeutics, Yingli Pharmaceuticals. Grants: Acerta Pharma, Agios, ArQule, Calithera Biosciences, Celgene, Constellation Pharmaceuticals, Curis, F. Hoffmann-
Figures

References
-
- McArthur GA, Chapman PB, Robert C, Larkin J, Haanen JB, Dummer R, et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014;15:323–32. doi: 10.1016/S1470-2045(14)70012-9. - DOI - PMC - PubMed
-
- Hochhaus A, Saglio G, Hughes TP, Larson RA, Kim DW, Issaragrisil S, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia. 2016;30:1044–54. doi: 10.1038/leu.2016.5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
