

Primary malignant melanomas of the female lower genital tract: clinicopathological characteristics and management
- PMID: 33414983
- PMCID: PMC7783736
Primary malignant melanomas of the female lower genital tract: clinicopathological characteristics and management
Abstract
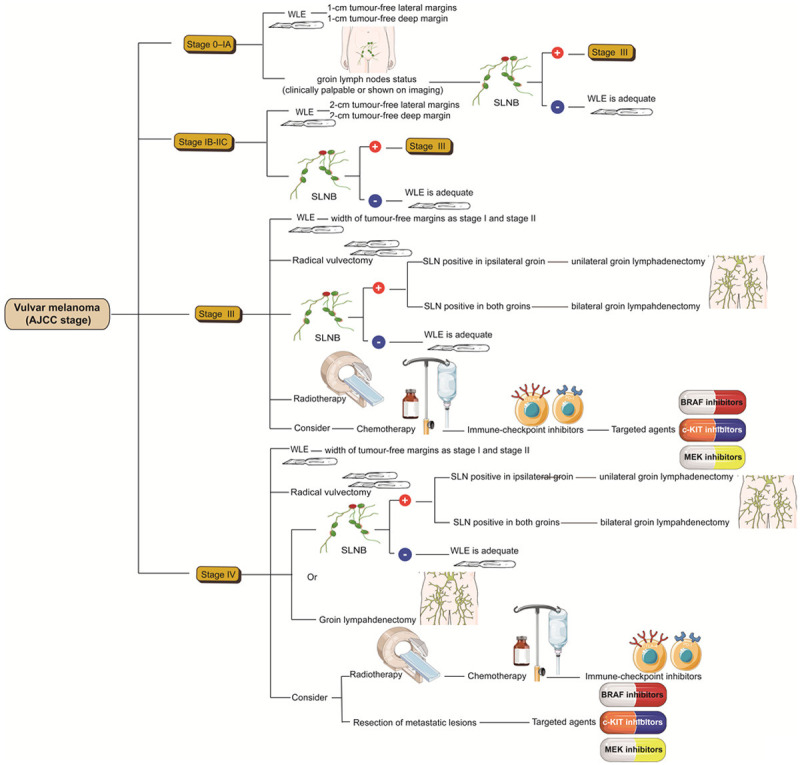
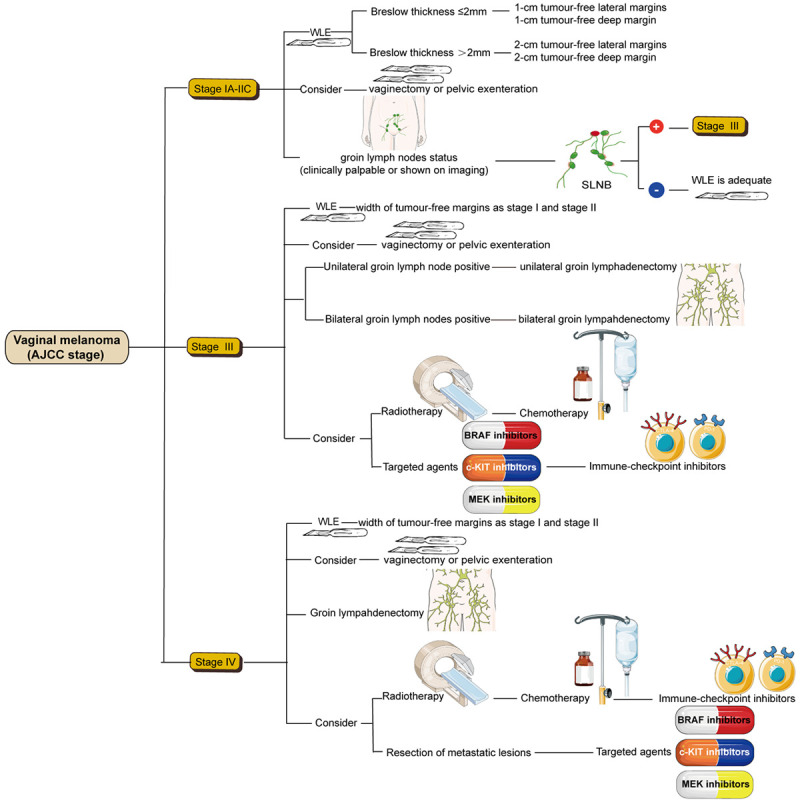
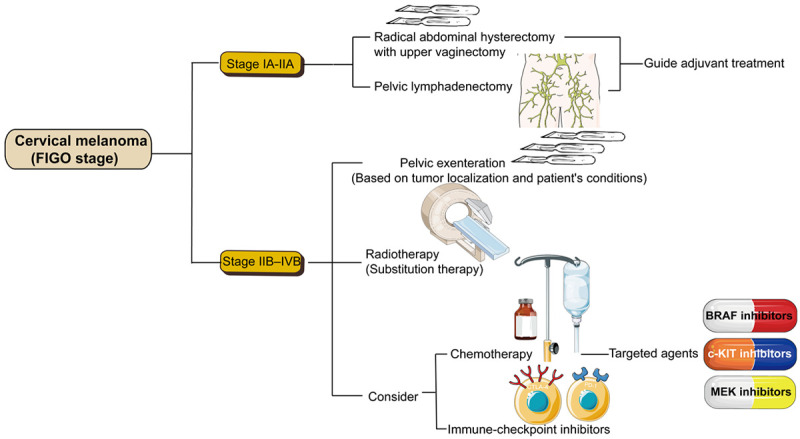
The female lower genital tract melanomas mainly include vulvar, vaginal and cervical melanoma. There is little clinical data on the melanomas thus making them highly lethal with their prognosis being worse than for cutaneous melanoma and other gynecological malignancies. Surgery is still the primary treatment for gynecological melanomas with wide local resection (WLE) of tumors with adequate margins being preferred for early-stage vulvar melanoma while complete resection of the primary tumor is the standard treatment for early-stage cervical and vaginal melanoma. Sentinel lymph node biopsy seems to avoid unnecessary complete regional lymphadenectomy. However, it should be chosen cautiously. Recently discovered molecular changes have provided new hopes for effective systemic treatment of female genital tract melanomas. In this review, we summarize the pathogenesis and clinicopathological characteristics of these rare melanomas with particular emphasis on new therapies and clinical management methods that may affect prognosis. The review aims to provide a viable direction for clinicians to diagnose and treat female lower genital tract melanomas.
Keywords: Vulva; cervix; diagnosis; malignant melanoma; prognosis; target therapy; vagina.
AJCR Copyright © 2020.
Conflict of interest statement
None.
Figures
Similar articles
-
Malignant Melanoma of the Female Genital Tract: Experience of an Oncology Center in Pakistan.Cureus. 2020 Jun 7;12(6):e8484. doi: 10.7759/cureus.8484. Cureus. 2020. PMID: 32642388 Free PMC article.
-
Management of melanomas of the female genital tract.Curr Opin Oncol. 2008 Sep;20(5):565-9. doi: 10.1097/CCO.0b013e32830b0dda. Curr Opin Oncol. 2008. PMID: 19106662 Review.
-
Female Genital Tract Melanoma: 10 Years of Experience at a Single Tertiary Center.J Low Genit Tract Dis. 2021 Apr 1;25(2):142-145. doi: 10.1097/LGT.0000000000000591. J Low Genit Tract Dis. 2021. PMID: 33587530
-
The role of sentinel lymph node mapping in lower genital tract melanoma.Minerva Ginecol. 2020 Dec;72(6):384-390. doi: 10.23736/S0026-4784.20.04628-6. Epub 2020 Aug 3. Minerva Ginecol. 2020. PMID: 32744452 Review.
-
Primary malignant melanoma of the female genital tract.Taiwan J Obstet Gynecol. 2009 Jun;48(2):169-75. doi: 10.1016/S1028-4559(09)60281-3. Taiwan J Obstet Gynecol. 2009. PMID: 19574182
Cited by
-
Successful treatment of metastatic vulvar malignant melanoma with toripalimab: A rare case report and review of the literature.Medicine (Baltimore). 2022 Sep 9;101(36):e30239. doi: 10.1097/MD.0000000000030239. Medicine (Baltimore). 2022. PMID: 36086787 Free PMC article. Review.
-
Primary Vaginal Amelanotic Melanoma: A Diagnostic Conundrum.Cureus. 2021 Dec 29;13(12):e20796. doi: 10.7759/cureus.20796. eCollection 2021 Dec. Cureus. 2021. PMID: 35141058 Free PMC article.
-
Long-term response of vulvar mucosal melanoma treated with neoadjuvant nivolumab.JAAD Case Rep. 2023 Jun 8;38:14-16. doi: 10.1016/j.jdcr.2023.05.037. eCollection 2023 Aug. JAAD Case Rep. 2023. PMID: 37600735 Free PMC article. No abstract available.
-
Surgical Management of Vulvar Melanoma: A Case Series.Case Rep Oncol. 2021 Jul 20;14(2):1144-1151. doi: 10.1159/000517820. eCollection 2021 May-Aug. Case Rep Oncol. 2021. PMID: 34413746 Free PMC article.
-
Gynecologic tract melanoma in the contemporary therapeutic era: High rates of local and distant disease progression.Gynecol Oncol. 2022 Dec;167(3):483-489. doi: 10.1016/j.ygyno.2022.09.026. Epub 2022 Oct 11. Gynecol Oncol. 2022. PMID: 36229264 Free PMC article.
References
-
- Rastrelli M, Tropea S, Rossi CR, Alaibac M. Melanoma: epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo. 2014;28:1005–1011. - PubMed
-
- McLaughlin CC, Wu XC, Jemal A, Martin HJ, Roche LM, Chen VW. Incidence of noncutaneous melanomas in the U.S. Cancer. 2005;103:1000–1007. - PubMed
-
- Gong HZ, Zheng HY, Li J. Amelanotic melanoma. Melanoma Res. 2019;29:221–230. - PubMed
-
- Khurana A, Jalpota Y. Primary malignant melanoma of the uterine cervix. Indian J Pathol Microbiol. 2009;52:575–576. - PubMed
Publication types
LinkOut - more resources
Full Text Sources