

Comparison of the Efficacy of the Various Treatment Modalities in the Management of Perianal Crohn's Fistula: A Review
- PMID: 33415035
- PMCID: PMC7781784
- DOI: 10.7759/cureus.11882
Comparison of the Efficacy of the Various Treatment Modalities in the Management of Perianal Crohn's Fistula: A Review
Abstract
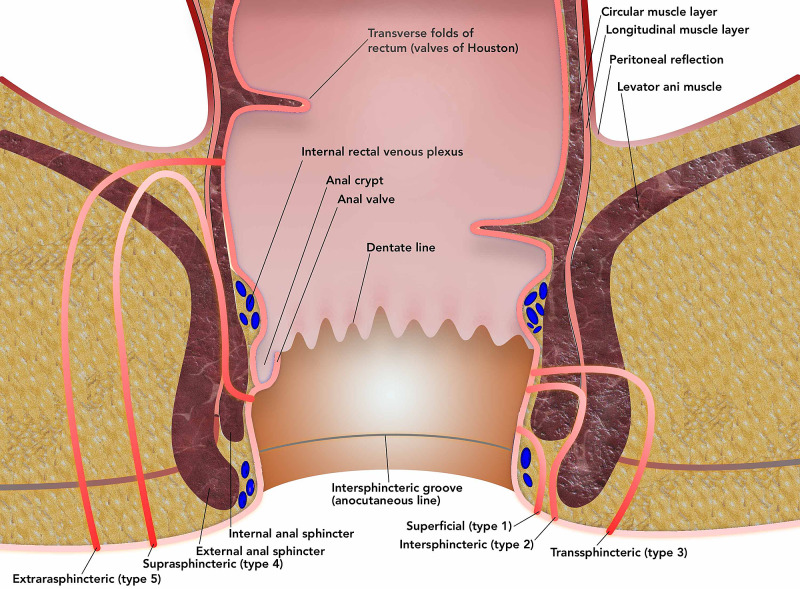
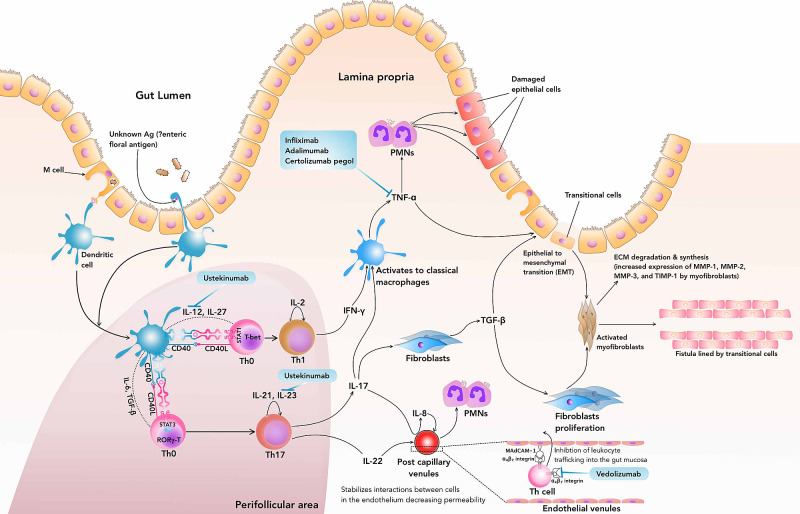
Crohn's disease (CD) is a transmural inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal (GI) tract. With the disease's progression, adhesions and transmural fissuring, intra-abdominal abscesses, and fistula tracts may develop. An anal fistula (or fistula-in-ano) is a chronic abnormal epithelial lined tract communicating the anorectal lumen (internal opening) to the perineal or buttock skin (external opening). The risk of fistula development varies from 14%-38%. It can cause significant morbidity, which adversely impacts the quality of life. It is mostly believed that an anal crypt gland infection causes anal abscesses, leading to fistula development. Crohn's disease's pathogenesis involves Th1 and Th17 hypersensitivity due to an unknown antigen within the intestinal mucosa. Evidence to support this review was gathered via the Pubmed database. Search terms used were combinations of "Perianal fistula," "seton," "immunotherapy." Studies were reviewed and cross-referenced for additional reports. Setons are surgical thread loops passed from the external to the internal opening of the fistula tract and exteriorized through the anorectal canal, facilitating abscess drainage and inciting a local inflammatory reaction, thus promoting the resolution of the fistula. Biologicals such as anti-tumor necrosis factor (TNF) antibody (infliximab, adalimumab, certolizumab), anti-IL-12/23 (ustekinumab), and anti-α₄β₇ integrin antibody (vedolizumab) have been approved for Crohn's disease targeting the Th1/Th17-mediated inflammation. Other therapeutic modalities are fistulotomy, cyanoacrylate glue, bioprosthetic plugs, mucosal advancement flap, ligation of inter-sphincteric fistula tract (LIFT), diverting stoma, proctectomy, video-assisted anal fistula treatment (VAAFT), and fistula laser closure (FiLaC). Our review found that chronic seton therapy should be the primary approach, especially if the patient has a perianal abscess. It has a low incidence of re-intervention, recurrent abscess formation, and side-branching of the fistulous tract, with preservation of the fistulous tract's patency and cost-effectiveness. The major disadvantage of seton therapy is the discomfort and time to achieve stability. Among the biologicals, infliximab is the only therapy which has a statistically significant effect on the healing rate of perianal Crohn's fistula compared to placebo, but the major disadvantage associated with anti-TNF as sole therapy is high re-intervention rate, prolong maintenance therapy, high recurrence rate, and severe side effects. We hypothesize that the two aspects should be addressed concurrently to increase the fistula healing or closure rate. First, the seton should be used as initial therapy to maintain tract patency to allow abscess drainage and minimize the intestinal flora colonization within the tract mucosa, thereby leukocytic infiltration and propagation of inflammation within the tract. The second aspect that has to be considered is that we should target the initial stimulation of the Th1/Th17 mediated hypersensitivity instead of a factor/cytokine involved in the inflammation mediation. Although the unknown antigen triggering such hypersensitivity is not clear, we could target the RAR-related orphan receptor γ (RORγ)-T (transcription factor involved in activation of Th17 cells) and the T-bet (transcription factor involved in activation of Th17 cells) within the GI mucosa by a novel target immune therapy.
Keywords: biologicals; crohn's disease; fistulotomy; infliximab; perianal fistula; seton; ustekinumab; vedolizumab.
Copyright © 2020, Feroz et al.
Conflict of interest statement
All the images included in the review article.
Figures

References
-
- The role of loose seton in the management of anal fistula: a multicenter study of 200 patients. Kelly ME, Heneghan HM, McDermott FD, Nason GJ, Freeman C, Martin ST, Winter DC. Tech Coloproctol. 2014;18:915–919. - PubMed
-
- Prevalence of inflammatory bowel disease among adults aged ≥18 years—United States, 2015. [Oct;2020 ];Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB. MMWR Morb Mortal Wkly Rep. 2015 65:1166–1169. - PubMed
-
- National estimates of the burden of inflammatory bowel disease among racial and ethnic groups in the United States. Nguyen GC, Chong CA, Chong RY. J Crohns Colitis. 2014;8:288–295. - PubMed
Publication types
LinkOut - more resources
Full Text Sources