

Risk Factors for Atonic Postpartum Hemorrhage: A Systematic Review and Meta-analysis
- PMID: 33417319
- PMCID: PMC8336570
- DOI: 10.1097/AOG.0000000000004228
Risk Factors for Atonic Postpartum Hemorrhage: A Systematic Review and Meta-analysis
Abstract
Objective: To identify and quantify risk factors for atonic postpartum hemorrhage.
Data sources: PubMed, CINAHL, EMBASE, Web of Science, and and ClinicalTrials.gov databases were searched for English language studies with no restrictions on date or location. Studies included randomized trials, prospective or retrospective cohort studies, and case-control studies of pregnant patients who developed atonic postpartum hemorrhage and reported at least one risk factor.
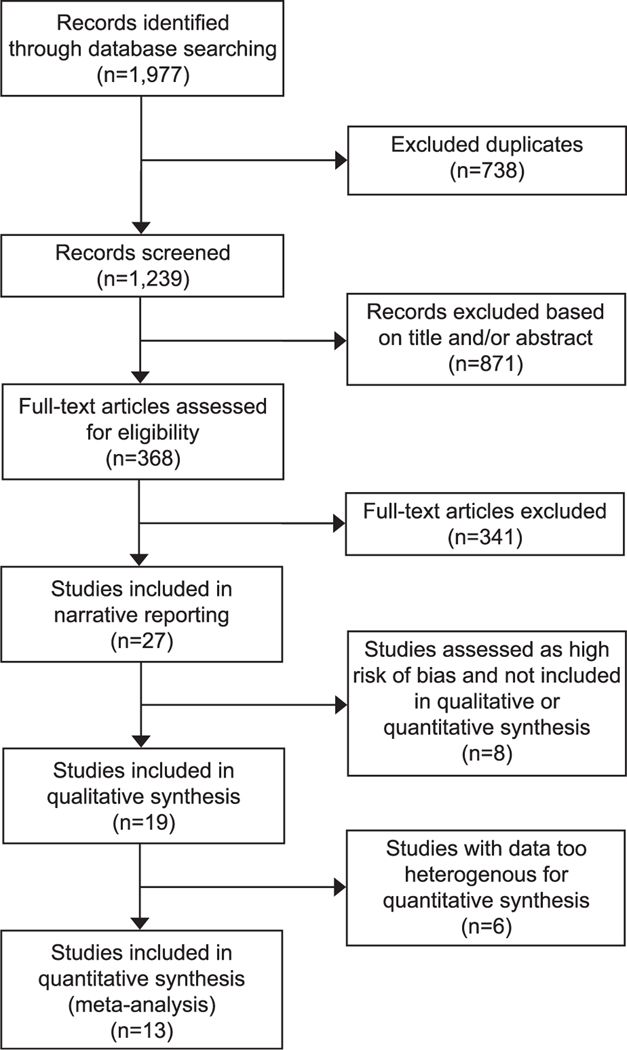
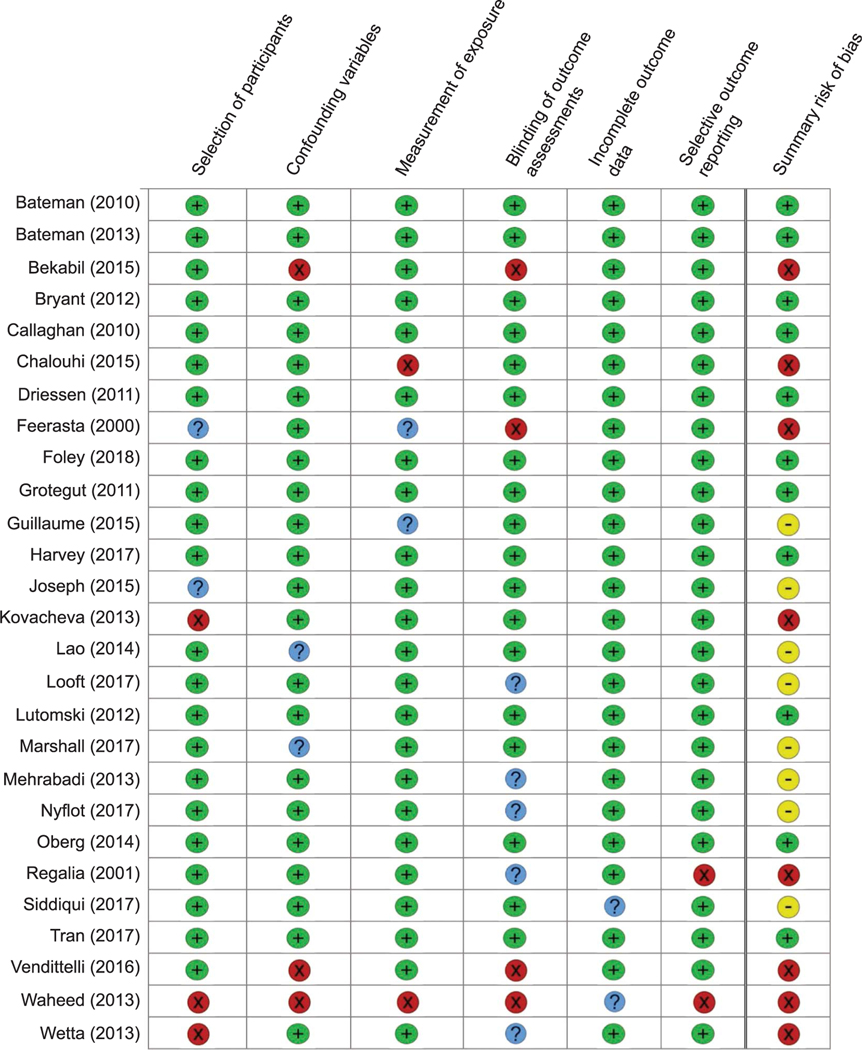
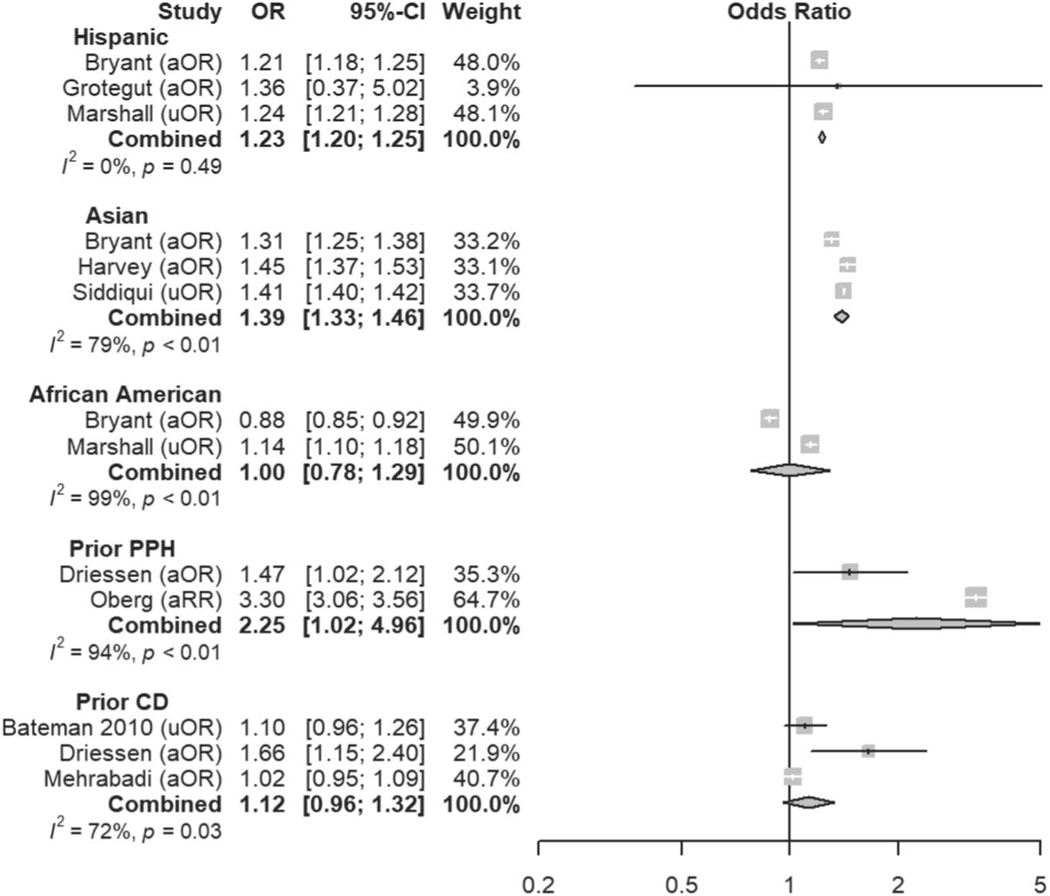
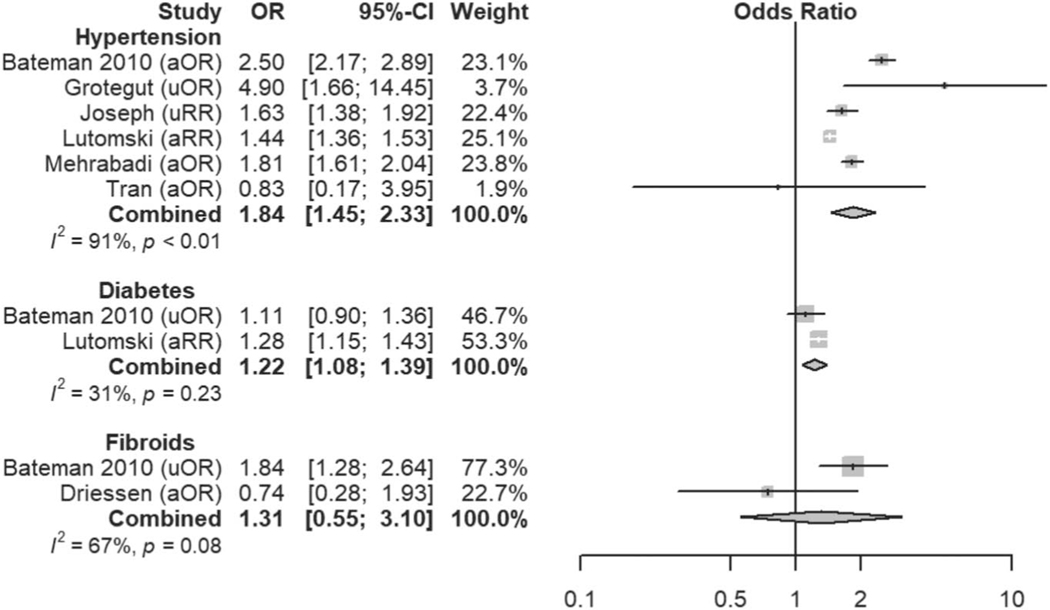
Methods of study selection: Title, abstract, and full-text screening were performed using the Raayan web application. Of 1,239 records screened, 27 studies were included in this review. Adjusted or unadjusted odds ratios (ORs), relative risks, or rate ratios were recorded or calculated. For each risk factor, a qualitative synthesis of low and moderate risk of bias studies classifies the risk factor as definite, likely, unclear, or not a risk factor. For risk factors with sufficiently homogeneous definitions and reference ranges, a quantitative meta-analysis of low and moderate risk of bias studies was implemented to estimate a combined OR.
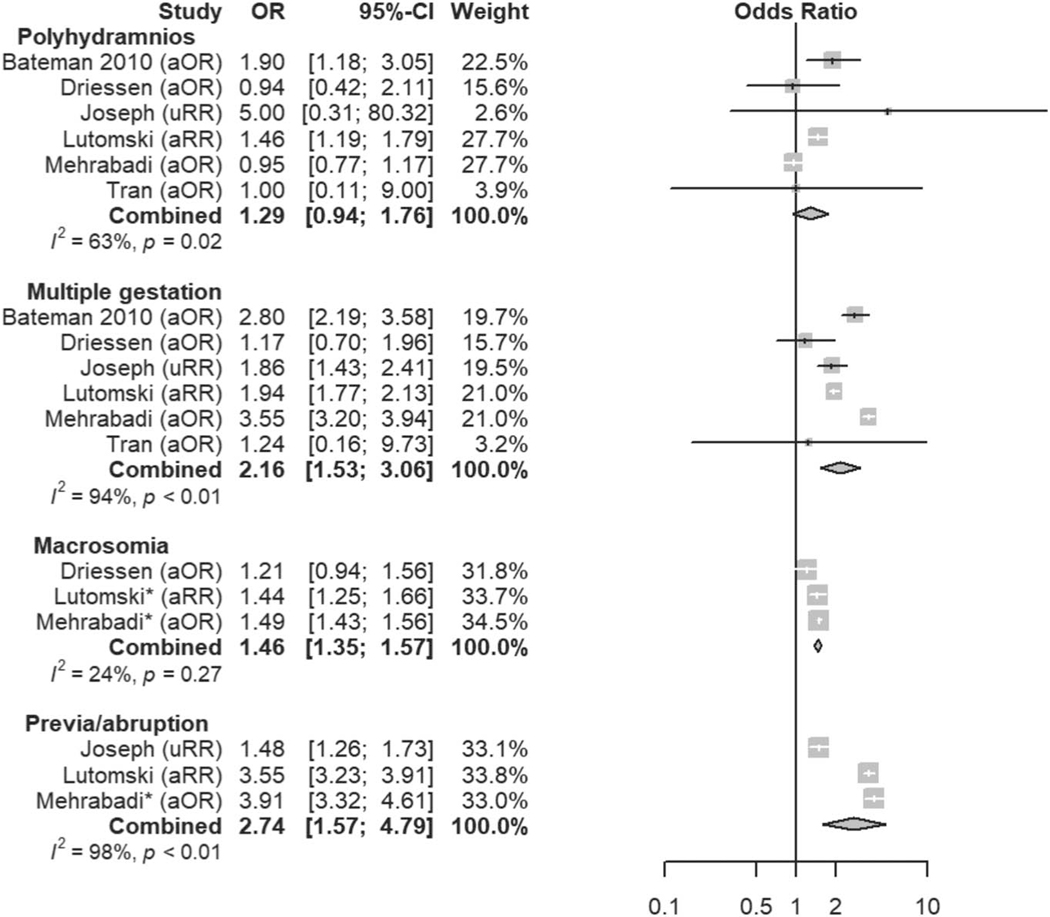
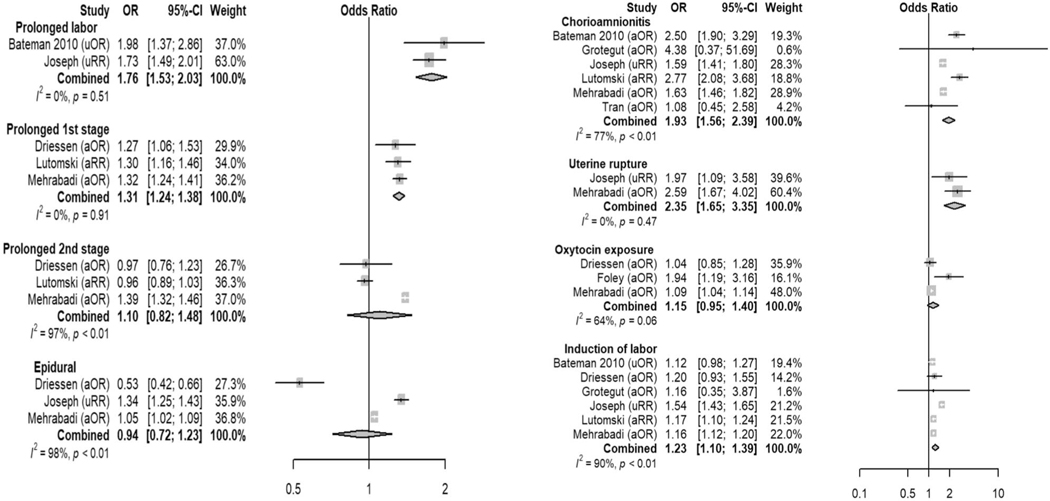
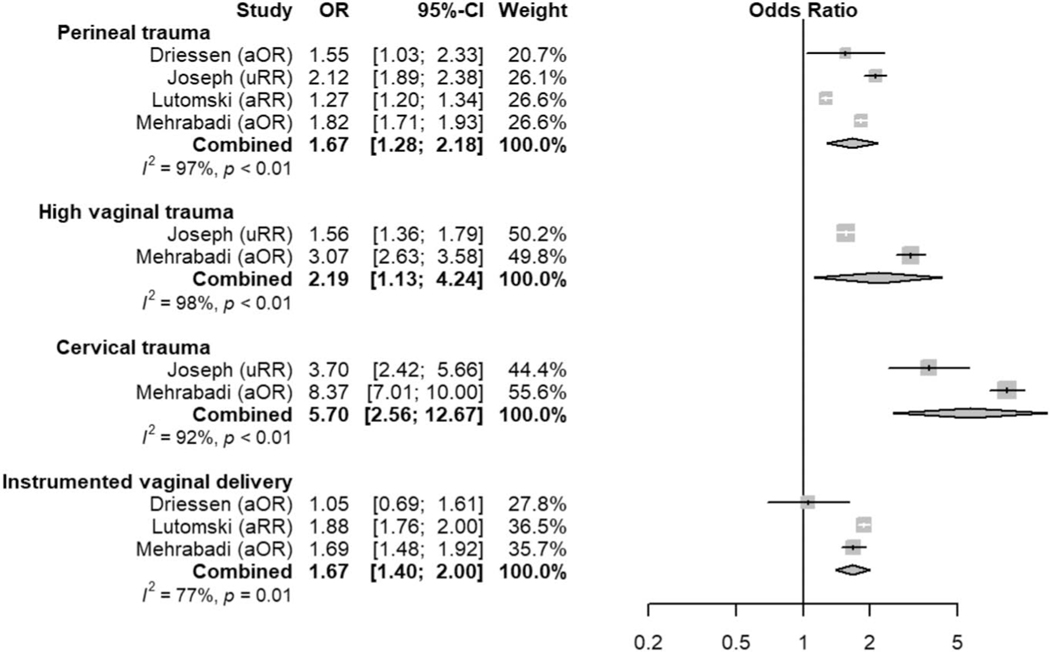
Tabulation, integration, and results: Forty-seven potential risk factors for atonic postpartum hemorrhage were identified in this review, of which 15 were judged definite or likely risk factors. The remaining 32 assessed risk factors showed no association with atonic postpartum hemorrhage or had conflicting or unclear evidence.
Conclusion: A substantial proportion of postpartum hemorrhage occurs in the absence of recognized risk factors. Many risk factors for atonic hemorrhage included in current risk-assessment tools were confirmed, with the greatest risk conferred by prior postpartum hemorrhage of any etiology, placenta previa, placental abruption, uterine rupture, and multiple gestation. Novel risk factors not currently included in risk-assessment tools included hypertension, diabetes, and ethnicity. Obesity and magnesium were not associated with atonic postpartum hemorrhage in this review.
Systematic review registration: PROSPERO, CRD42020157521.
Copyright © 2021 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure The authors did not report any potential conflicts of interest.
Figures
Similar articles
-
Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis.Am J Obstet Gynecol. 2020 Apr;222(4):293.e1-293.e52. doi: 10.1016/j.ajog.2019.11.1287. Epub 2020 Jan 6. Am J Obstet Gynecol. 2020. PMID: 31917139
-
Causes of and risk factors for postpartum haemorrhage: a systematic review and meta-analysis.Lancet. 2025 Apr 26;405(10488):1468-1480. doi: 10.1016/S0140-6736(25)00448-9. Epub 2025 Apr 3. Lancet. 2025. PMID: 40188841
-
Exaggerated placental site, consisting of implantation site intermediate trophoblasts, causes massive postpartum uterine hemorrhage: case report and literature review.Tohoku J Exp Med. 2014 Sep;234(1):77-82. doi: 10.1620/tjem.234.77. Tohoku J Exp Med. 2014. PMID: 25186195 Review.
-
The association between maternal vitamin D deficiency and postpartum hemorrhage and uterine atony.Acta Obstet Gynecol Scand. 2024 Feb;103(2):286-293. doi: 10.1111/aogs.14719. Epub 2023 Nov 14. Acta Obstet Gynecol Scand. 2024. PMID: 37960966 Free PMC article.
-
Increasing trends in atonic postpartum haemorrhage in Ireland: an 11-year population-based cohort study.BJOG. 2012 Feb;119(3):306-14. doi: 10.1111/j.1471-0528.2011.03198.x. Epub 2011 Dec 13. BJOG. 2012. PMID: 22168794
Cited by
-
Culturally adapted flowcharts in obstetric emergencies: a participatory action research study.BMC Pregnancy Childbirth. 2022 Oct 14;22(1):772. doi: 10.1186/s12884-022-05105-z. BMC Pregnancy Childbirth. 2022. PMID: 36229785 Free PMC article.
-
Comparison of Clinical Efficacy and Safety between Misoprostol and Oxytocin in the Prevention of Postpartum Hemorrhage: A Meta-Analysis.J Healthc Eng. 2022 Apr 11;2022:3254586. doi: 10.1155/2022/3254586. eCollection 2022. J Healthc Eng. 2022. Retraction in: J Healthc Eng. 2023 Oct 4;2023:9895282. doi: 10.1155/2023/9895282. PMID: 35449871 Free PMC article. Retracted.
-
Health care provider decision-making and the quality of maternity care: An analysis of postpartum care in Kenyan hospitals.Soc Sci Med. 2023 Aug;331:116071. doi: 10.1016/j.socscimed.2023.116071. Epub 2023 Jul 4. Soc Sci Med. 2023. PMID: 37450989 Free PMC article.
-
Does induction or augmentation of labor increase the risk of postpartum hemorrhage in pregnant women with anemia? A multicenter prospective cohort study in India.Int J Gynaecol Obstet. 2025 Apr;169(1):299-309. doi: 10.1002/ijgo.16008. Epub 2024 Nov 8. Int J Gynaecol Obstet. 2025. PMID: 39513665 Free PMC article.
-
Maternal, Perinatal and Neonatal Outcomes of Triplet Pregnancies According to Chorionicity: A Systematic Review of the Literature and Meta-Analysis.J Clin Med. 2022 Mar 28;11(7):1871. doi: 10.3390/jcm11071871. J Clin Med. 2022. PMID: 35407479 Free PMC article.
References
-
- Bingham D, Melsop K, Main E. CMQCC Obstetric hemorrhage hospital level implementation guide. Stanford University; 2010
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
