

Proteogenomic insights into the biology and treatment of HPV-negative head and neck squamous cell carcinoma
- PMID: 33417831
- PMCID: PMC7946781
- DOI: 10.1016/j.ccell.2020.12.007
Proteogenomic insights into the biology and treatment of HPV-negative head and neck squamous cell carcinoma
Abstract
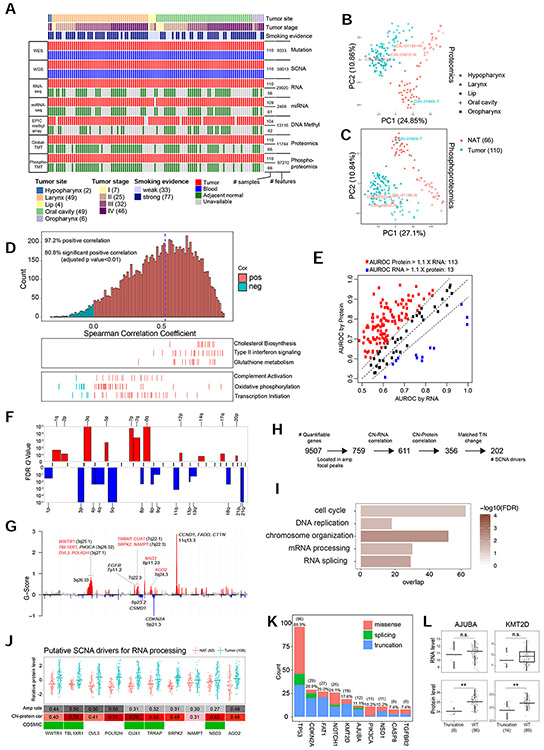
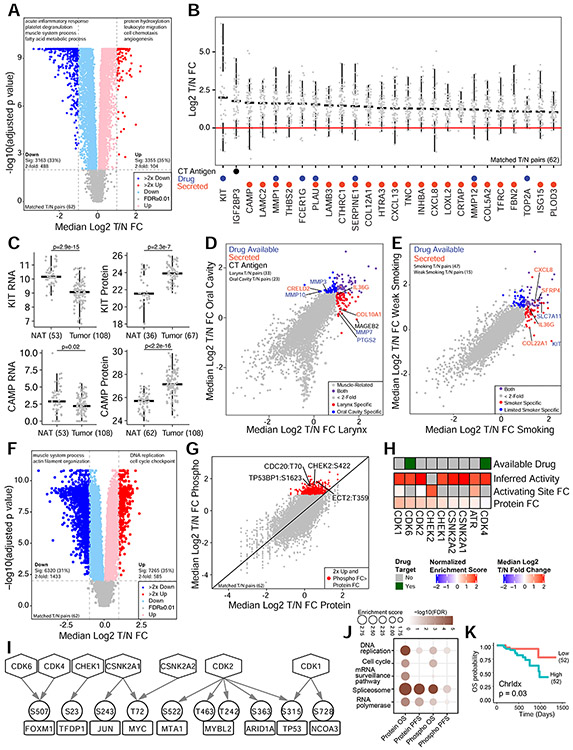
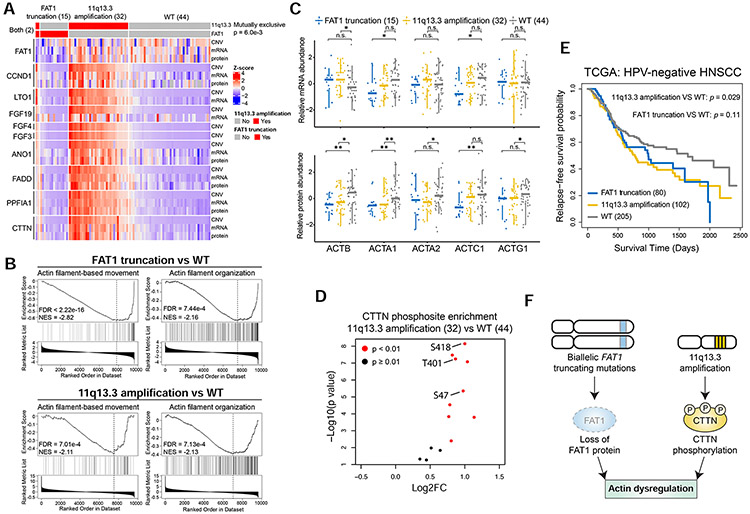
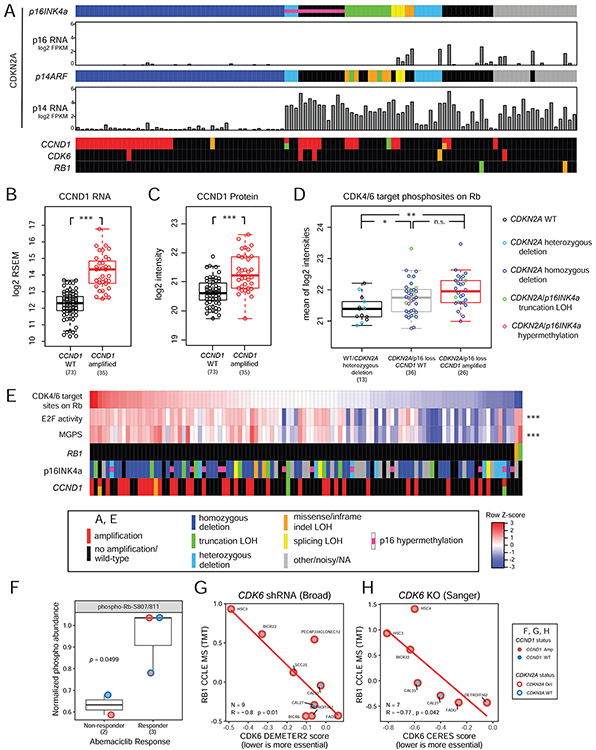
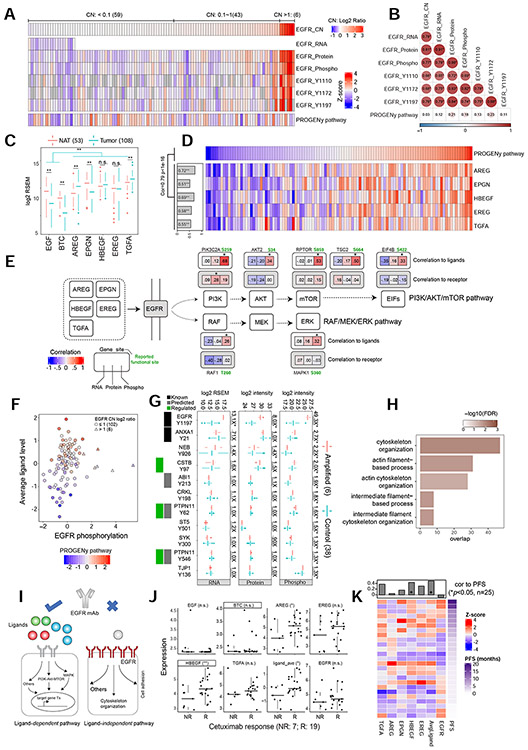
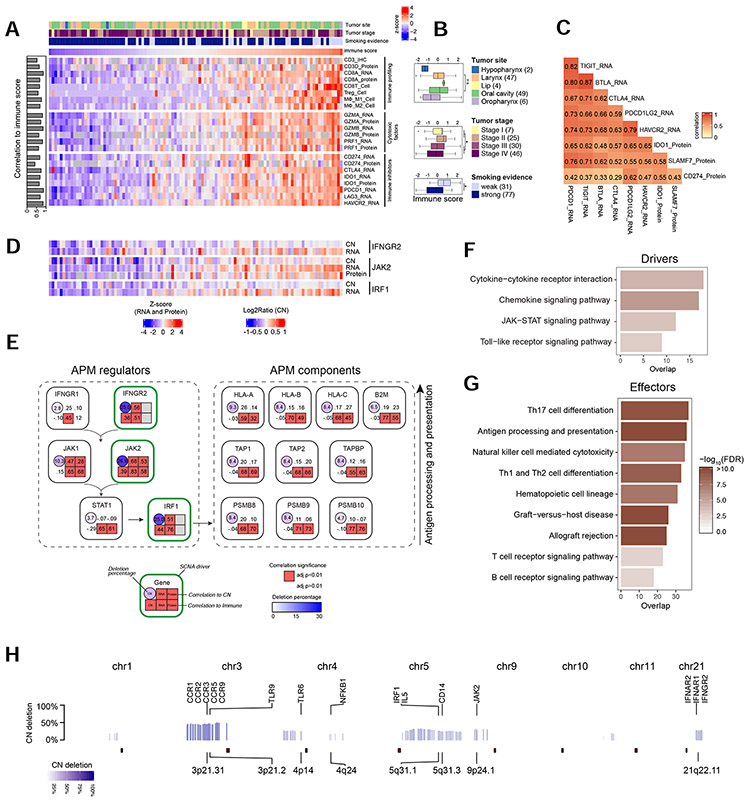
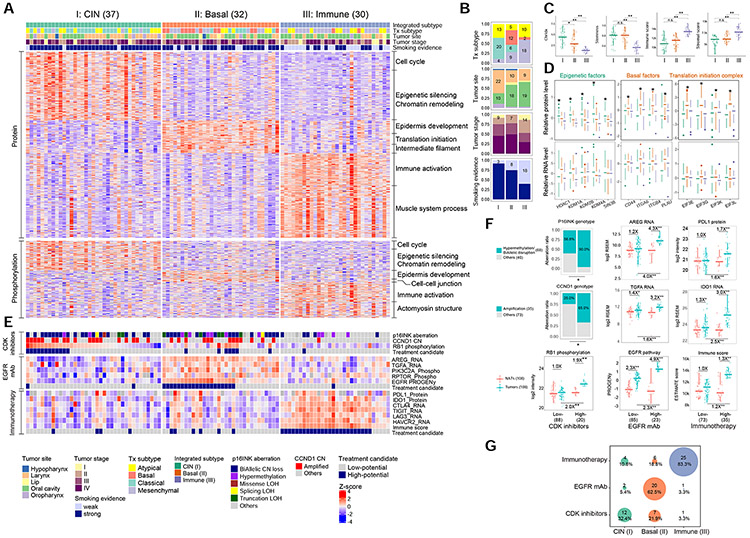
We present a proteogenomic study of 108 human papilloma virus (HPV)-negative head and neck squamous cell carcinomas (HNSCCs). Proteomic analysis systematically catalogs HNSCC-associated proteins and phosphosites, prioritizes copy number drivers, and highlights an oncogenic role for RNA processing genes. Proteomic investigation of mutual exclusivity between FAT1 truncating mutations and 11q13.3 amplifications reveals dysregulated actin dynamics as a common functional consequence. Phosphoproteomics characterizes two modes of EGFR activation, suggesting a new strategy to stratify HNSCCs based on EGFR ligand abundance for effective treatment with inhibitory EGFR monoclonal antibodies. Widespread deletion of immune modulatory genes accounts for low immune infiltration in immune-cold tumors, whereas concordant upregulation of multiple immune checkpoint proteins may underlie resistance to anti-programmed cell death protein 1 monotherapy in immune-hot tumors. Multi-omic analysis identifies three molecular subtypes with high potential for treatment with CDK inhibitors, anti-EGFR antibody therapy, and immunotherapy, respectively. Altogether, proteogenomics provides a systematic framework to inform HNSCC biology and treatment.
Keywords: CDK inhibitor; CPTAC; EGFR mAb; HNSCC; combination immune checkpoint blockade; immune evasion; immunotherapy; predictive biomarker; proteogenomics; proteomics.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests S.A.C. is a member of the scientific advisory boards of Kymera, PTM BioLabs, and Seer and a scientific advisor to Pfizer and Biogen. The other authors have no conflicts of interest to declare. M.J.E. reports ownership and royalties associated with Bioclassifier LLC through sales by Nanostring LLC and Veracyte for the "Prosigna" breast cancer prognostic test. M.J.E. also reports ad hoc consulting for AstraZeneca, Foundation Medicine, G1 Therapeutics, Novartis, Sermonix, Abbvie, Lilly and Pfizer.
Figures
References
-
- Adkins D, Ley J, Neupane P, Worden F, Sacco AG, Palka K, Grilley-Olson JE, Maggiore R, Salama NN, Trinkaus K, et al. (2019). Palbociclib and cetuximab in platinum-resistant and in cetuximab-resistant human papillomavirus-unrelated head and neck cancer: a multicentre, multigroup, phase 2 trial. Lancet Oncol 20, 1295–1305. - PubMed
-
- Ang KK, Zhang Q, Rosenthal DI, Nguyen-Tan PF, Sherman EJ, Weber RS, Galvin JM, Bonner JA, Harris J, El-Naggar AK, et al. (2014). Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J Clin Oncol 32, 2940–2950. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
