

Umbilical Cord Milking vs Delayed Cord Clamping and Associations with In-Hospital Outcomes among Extremely Premature Infants
- PMID: 33417919
- PMCID: PMC8084979
- DOI: 10.1016/j.jpeds.2020.12.072
Umbilical Cord Milking vs Delayed Cord Clamping and Associations with In-Hospital Outcomes among Extremely Premature Infants
Abstract
Objective: To compare in-hospital outcomes after umbilical cord milking vs delayed cord clamping among infants <29 weeks of gestation.
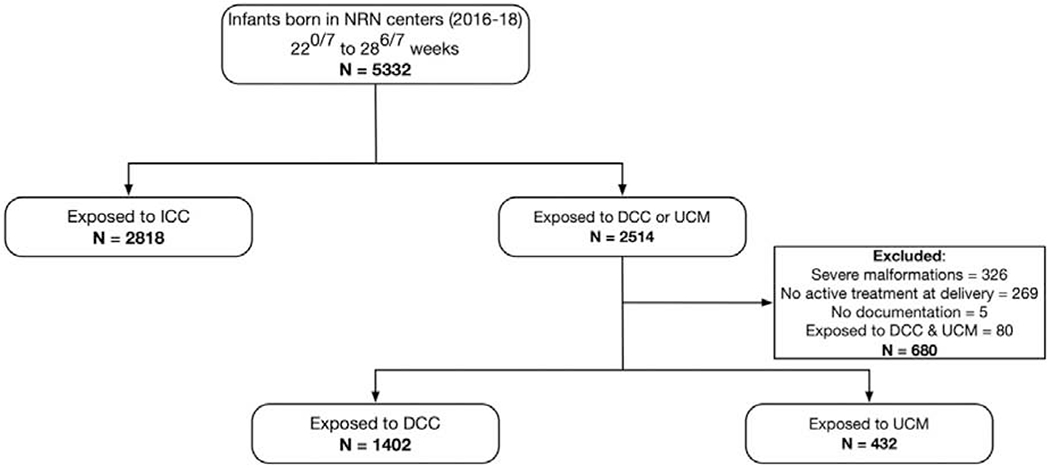
Study design: Multicenter retrospective study of infants born <29 weeks of gestation from 2016 to 2018 without congenital anomalies who received active treatment at delivery and were exposed to umbilical cord milking or delayed cord clamping. The primary outcome was mortality or severe (grade III or IV) intraventricular hemorrhage (IVH) by 36 weeks of postmenstrual age (PMA). Secondary outcomes assessed at 36 weeks of PMA were mortality, severe IVH, any IVH or mortality, and a composite of mortality or major morbidity. Outcomes were assessed using multivariable regression, incorporating mortality risk factors identified a priori, confounders, and center. A prespecified, exploratory analysis evaluated severe IVH in 2 gestational age strata, 22-246/7 and 25-286/7 weeks.
Results: Among 1834 infants, 23.6% were exposed to umbilical cord milking and 76.4% to delayed cord clamping. The primary outcome, mortality or severe IVH, occurred in 21.1% of infants: 28.3% exposed to umbilical cord milking and 19.1% exposed to delayed cord clamping, with an aOR that was similar between groups (aOR 1.45, 95% CI 0.93, 2.26). Infants exposed to umbilical cord milking had higher odds of severe IVH (19.8% umbilical cord milking vs 11.8% delayed cord clamping, aOR 1.70 95% CI 1.20, 2.43), as did the 25-286/7 week stratum (14.8% umbilical cord milking vs 7.4% delayed cord clamping, aOR 1.89 95% CI 1.22, 2.95). Other secondary outcomes were similar between groups.
Conclusions: This analysis of extremely preterm infants suggests that delayed cord clamping is the preferred practice for placental transfusion, as umbilical cord milking exposure was associated with an increase in the adverse outcome of severe IVH.
Trial registration: ClinicalTrials.gov: NCT00063063.
Keywords: Neonatal Research Network; intraventricular hemorrhage; placental transfusion.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures


References
-
- Rabe H, Gyte GM, Díaz-Rossello JL, Duley L. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database of Systematic Reviews 2019; 9 Available from: http://doi.wiley.com/10.1002/14651858.CD003248.pub4 - DOI - PMC - PubMed
-
- American Academy of Pediatrics. Timing of umbilical cord clamping after birth. Pediatrics 2013; April 1;131: e1323–e1323. DOI: 10.1542/peds.2013-0191 - DOI
-
- Perlman JM, Wyllie J, Kattwinkel J, Wyckoff MH, Aziz K, Guinsburg R, et al. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations (Reprint). Pediatrics 2015; November 1;136: S120–66. doi:10.1542/peds.2015-3373D - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
