

Molecular Pathogenesis and Treatment Perspectives for Hypereosinophilia and Hypereosinophilic Syndromes
- PMID: 33418988
- PMCID: PMC7825323
- DOI: 10.3390/ijms22020486
Molecular Pathogenesis and Treatment Perspectives for Hypereosinophilia and Hypereosinophilic Syndromes
Abstract
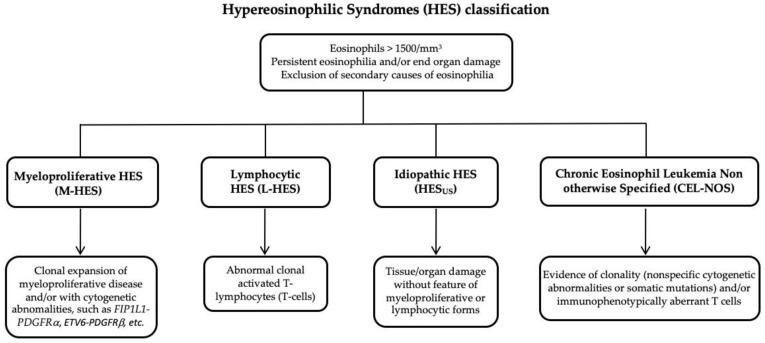
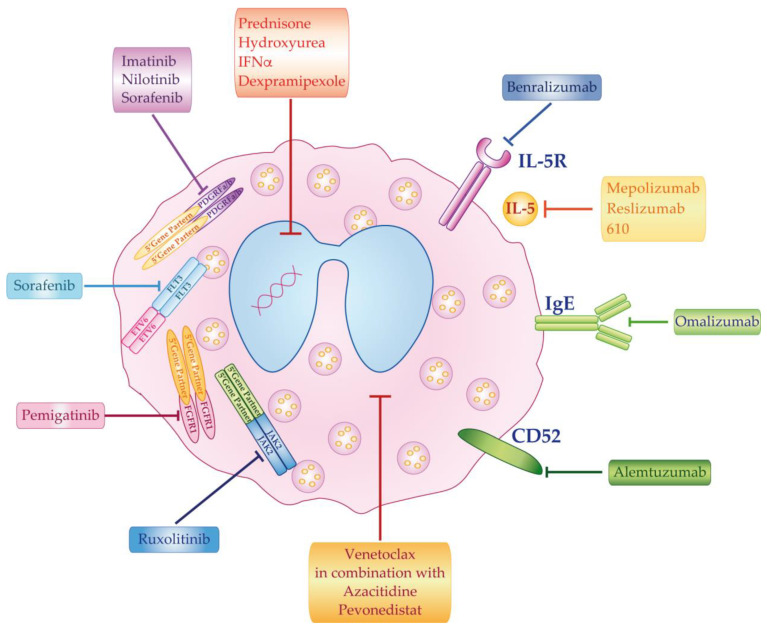
Hypereosinophilia (HE) is a heterogeneous condition with a persistent elevated eosinophil count of >350/mm3, which is reported in various (inflammatory, allergic, infectious, or neoplastic) diseases with distinct pathophysiological pathways. HE may be associated with tissue or organ damage and, in this case, the disorder is classified as hypereosinophilic syndrome (HES). Different studies have allowed for the discovery of two major pathogenetic variants known as myeloid or lymphocytic HES. With the advent of molecular genetic analyses, such as T-cell receptor gene rearrangement assays and Next Generation Sequencing, it is possible to better characterize these syndromes and establish which patients will benefit from pharmacological targeted therapy. In this review, we highlight the molecular alterations that are involved in the pathogenesis of eosinophil disorders and revise possible therapeutic approaches, either implemented in clinical practice or currently under investigation in clinical trials.
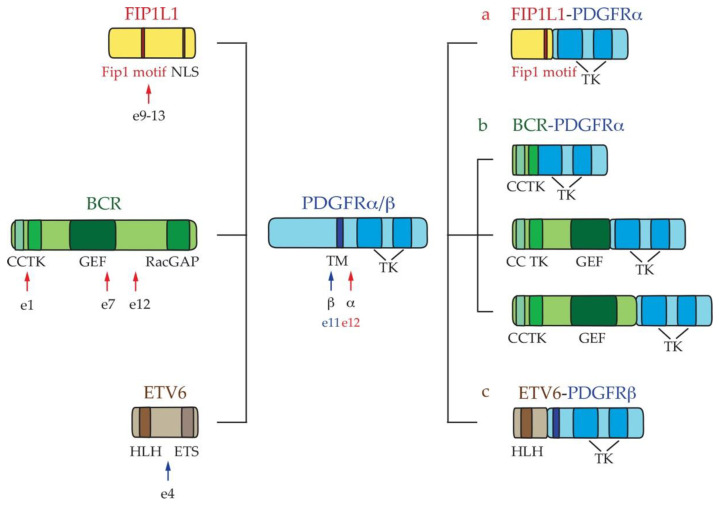
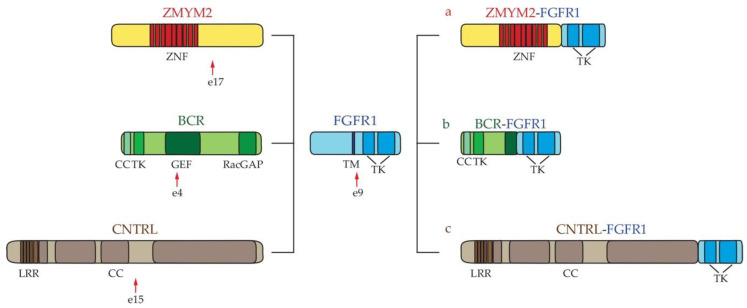
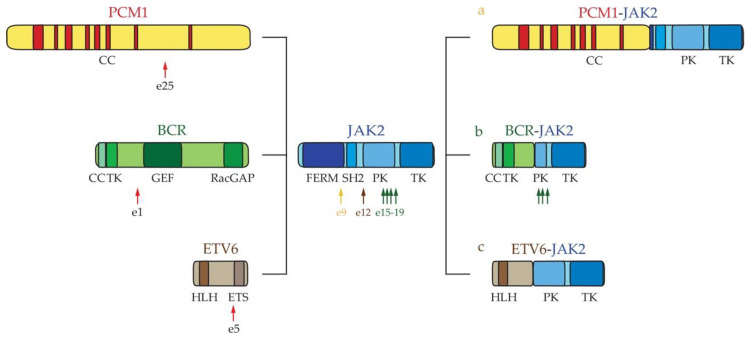
Keywords: NGS; PDGFRα and PDGFRβ fusions; TCR rearrangements; hypereosinophilia; hypereosinophilic syndromes.
Conflict of interest statement
Giuseppe Alberto Palumbo: homoraria from Novartis, Bristol Myers Squibb, Celgen, Amgen and Abbvie Paolo Vigneri: research funding from Novartis and Pfizer; honoraria from Astra-Zeneca, Celgene, Italfarmaco, Incyte, Novartis, Pfizer, Tesaro, and Teva. The other authors declare no conflict of interest.
Figures
References
-
- Dvorak A.M., Letourneau L., Login G.R., Weller P.F., Ackerman S.J. Ultrastructural localization of the Charcot-Leyden crystal protein (lysophospholipase) to a distinct crystalloid-free granule population in mature human eosinophils. Blood. 1988;72:150–158. doi: 10.1182/blood.V72.1.150.150. - DOI - PubMed
-
- Giembycz M.A., Lindsay M.A. Pharmacology of the eosinophil. Pharmacol. Rev. 1999;51:213–340. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
