

Myofascial Injection Using Fascial Layer-Specific Hydromanipulation Technique (FLuSH) and the Delineation of Multifactorial Myofascial Pain
- PMID: 33419263
- PMCID: PMC7766734
- DOI: 10.3390/medicina56120717
Myofascial Injection Using Fascial Layer-Specific Hydromanipulation Technique (FLuSH) and the Delineation of Multifactorial Myofascial Pain
Abstract
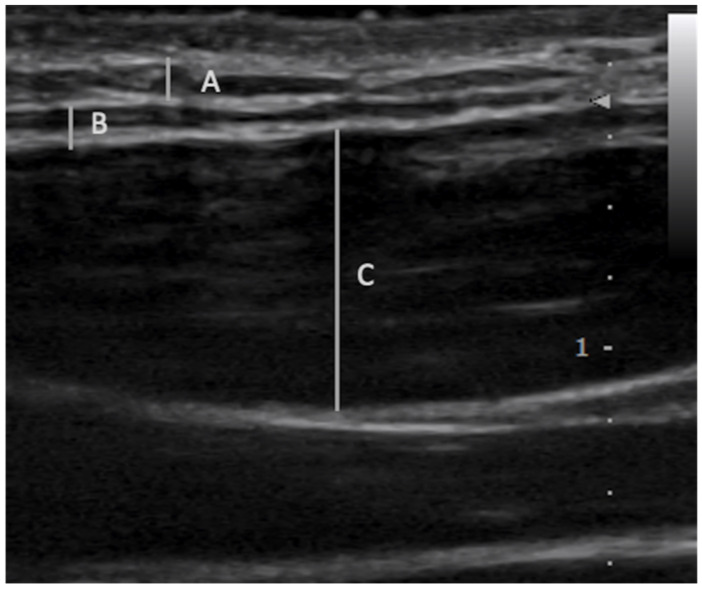
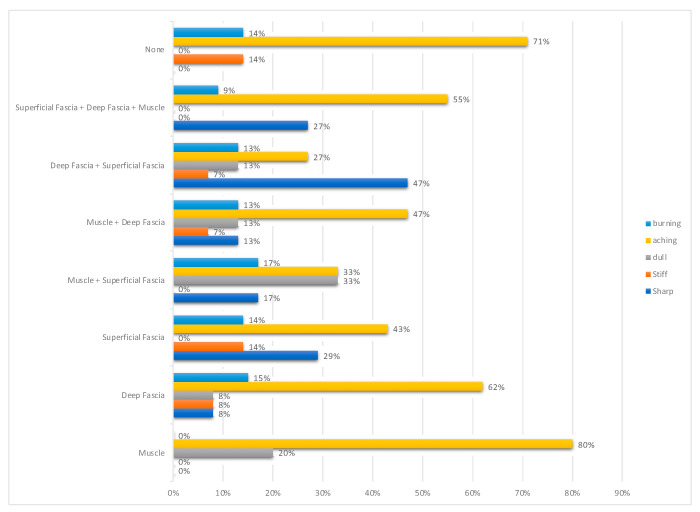
Background and objectives: The aims of this study were to delineate the contribution of specific fascial layers of the myofascial unit to myofascial pain and introduce the use of ultrasound-guided fascial layer-specific hydromanipulation (FLuSH) as a novel technique in the treatment of myofascial pain. Materials and Methods: The clinical data of 20 consecutive adult patients who underwent myofascial injections using FLuSH technique for the treatment of myofascial pain were reviewed. The FLuSH technique involved measuring the pain pressure threshold using an analog algometer initially and after each ultrasound guided injection of normal saline into the specific layers of the myofascial unit (superficial fascia, deep fascia, or muscle) in myofascial points corresponding with Centers of Coordination/Fusion (Fascial Manipulation®). The outcome measured was the change in pain pressure threshold after injection of each specific fascial layer. Results: Deep fascia was involved in 73%, superficial fascia in 55%, and muscle in 43% of points. A non-response to treatment of all three layers occurred in 10% of all injected points. The most common combinations of fascial layer involvement were deep fascia alone in 23%, deep fascia and superficial fascia in 22%, and deep fascia and muscle in 18% of injected points. Each individual had on average of 3.0 ± 1.2 different combinations of fascial layers contributing to myofascial pain. Conclusions: The data support the hypothesis that multiple fascial layers are responsible for myofascial pain. In particular, for a given patient, pain may develop from discrete combinations of fascial layers unique to each myofascial point. Non-response to treatment of the myofascial unit may represent a centralized pain process. Adequate treatment of myofascial pain may require treatment of each point as a distinct pathologic entity rather than uniformly in a given patient or across patients.
Keywords: fascia; injection; myofascial pain; myofascial unit; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Thomae M.K., Porteous J.E., Brock J.R., Allen G.D., Heller R.F. Back pain in Australian military helicopter pilots: A preliminary study. Aviat. Space Environ. Med. 1998;69:468–473. - PubMed
-
- Donnelly J.M., Simons D.G., editors. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. 3rd ed. Wolters Kluwer Health; Philadelphia, PA, USA: 2019. 935p
-
- Hua N.K., Van Der Does E. The occurrence and inter-rater reliability of myofascial trigger points in the quadratus lumborum and gluteus medius: A prospective study in non-specific low back pain patients and controls in general practice. Pain. 1994;58:317–323. doi: 10.1016/0304-3959(94)90125-2. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
